|
Case Report
Synchronous bilateral male breast cancer: A case report and review of literature
1 Medical Student, School of Medicine, University of California Irvine, Irvine, California, United States of America
2 MD, Resident Physician, Department of Surgery, Division of Surgical Oncology, University of California Irvine, Orange, California, United States of America
3 MD, MPH, Resident Physician, Department of Surgery, Division of Surgical Oncology, University of California Irvine, Orange, California, United States of America
4 Associate Clinical Professor, Department of Surgery, Division of Surgical Oncology, University of California Irvine, Orange, California, United States of America
Address correspondence to:
Erin Lin
DO, Associate Clinical Professor of Surgery, Division of Surgical Oncology, Department of Surgery, University of California, Irvine Medical Center, 3800 Chapman Ave, Suite 6200, Orange, CA 92868-3298,
United States of America
Message to Corresponding Author
Article ID: 100127Z12ND2023
Access full text article on other devices

Access PDF of article on other devices

How to cite this article
Dunn N, Nguyen PD, Yuen SW, Lin E. Synchronous bilateral male breast cancer: A case report and review of literature. J Case Rep Images Surg 2023;9(2):32–39.ABSTRACT
Introduction: Male synchronous bilateral breast cancer, defined as contralateral breast cancer diagnosed within 12 months of a previous breast cancer, is extraordinarily rare. This case report aims to provide improved understanding of the nuances in presentation, associated risk factors, and treatment options of synchronous bilateral male breast cancer.
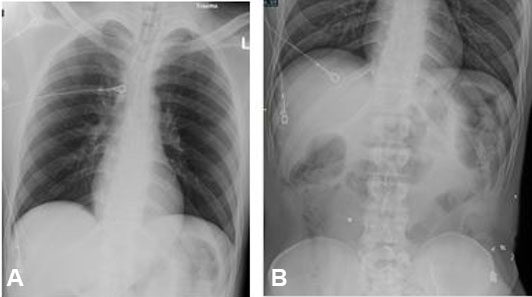
Case Report: A 68-year-old man presented with a one-month history of palpable bilateral retroareolar breast masses. He underwent workup with a bilateral breast ultrasound which showed an irregular hypoechoic mass 8 × 8 × 6 cm in the right breast at 7 o’clock in the retroareolar region and an oval hypoechoic mass 7 × 4 × 7 cm with indistinct margins in the left breast at 8 o’clock in the retroareolar region. Subsequent ultrasound-guided core needle biopsies revealed right breast moderately differentiated invasive ductal carcinoma and left breast high grade ductal carcinoma in situ. He underwent a bilateral simple mastectomy with bilateral axillary sentinel lymph node biopsies and was started on anastrozole at his initial post-operative visit. Four-month surveillance imaging with computed tomography chest, abdomen, pelvis, and dual X-ray absorptiometry showed no evidence of local recurrence or metastases.
Conclusion: Male breast cancer commonly presents as a painless retroareolar mass. Workup should include imaging studies to localize and characterize the lesion and tissue diagnosis via core needle biopsy. Treatment of male breast cancer largely includes simple mastectomy with adjuvant endocrine therapy. Future breast cancer studies should include male cohorts to improve our understanding and treatment options between the two sexes.
Keywords: Adjuvant endocrine therapy, Ductal carcinoma in situ, Invasive ductal carcinoma, Male breast cancer, Simple mastectomy, Synchronous bilateral breast cancer
SUPPORTING INFORMATION
Author Contributions
Natassia Dunn - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Peter D Nguyen - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Sarah W Yuen - Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
Erin Lin - Interpretation of data, Revising it critically for important intellectual content, Final approval of the version to be published
AcknowledgmentsThe authors do not have additional acknowledgments.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Natassia Dunn et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.