 |
Case Report
Pylephlebitis due to complicated diverticulitis: A case report and review of the literature
1 Medical Student, Central Michigan University, Mt Pleasant, Michigan, USA
2 General Surgery, Surgical Critical Care, MidMichigan Hospital, Midland, Michigan, USA
Address correspondence to:
Heather Cirotta
1632 Stone Street, Saginaw, Michigan 48602,
USA
Message to Corresponding Author
Article ID: 100064Z12CH2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cirotta H, Shah A. Pylephlebitis due to complicated diverticulitis: A case report and review of the literature. J Case Rep Images Surg 2019;5:100064Z12CH2019.ABSTRACT
Introduction: Pylephlebitis is a septic thrombophlebitis of the portal vein that is caused by intra-abdominal infection, most commonly diverticulitis. If the diagnosis is missed, the mortality can be high.
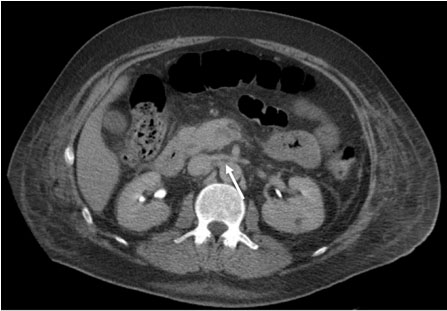
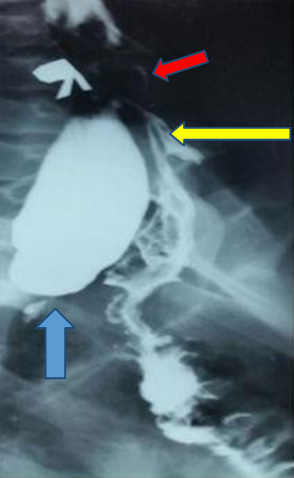
Case Report: A 49-year-old Caucasian man with past medical history (PMH) of gastroesophageal reflux disease (GERD), multiple episodes of diverticulitis, and alcoholism who presented to the emergency department (ED) with a three-week history of nausea, vomiting, and abdominal pain that had worsened over the last 24 hours. Baseline labs and vitals indicated severe sepsis and noncontrast computed tomography (CT) showed sigmoid diverticulitis with air within the mesenteric and portal veins. Clinically, the patient had exam findings consistent with localized peritonitis. The patient underwent exploratory laparotomy and Hartmann’s procedure for perforated diverticulitis and drainage of abscess. Concerns for pylephlebitis were suspected on postoperative day (POD) 7 due to patient’s increasing abdominal pain and large volume, serous Jackson–Pratt (JP) drainage. Thrombosis of superior mesenteric vein, main portal vein, right portal vein, and to lesser extent left portal vein was found on CT scan, suggestive of pylephlebitis. The patient was continued on intravenous (IV) antibiotics and started on systemic anticoagulation with improvement in his clinical condition.
Conclusion: Pylephlebitis is a suppurative thrombosis involving the veins that drain the abdomen and the portal venous system. It is most commonly a result of diverticulitis due to an increase inflammatory process and causes death in about 25% of patients. It is best diagnosed using CT with oral and IV contrast, and can be associated with portal venous gas. The mainstay of treatment is antibiotics, selection depending on the suspected source. The role of systemic anticoagulation is somewhat controversial as there is limited data to support its use.
Keywords: Diverticulitis, Portal venous gas, Pylephlebitis
Introduction
Pylephlebitis is a suppurative thrombophlebitis, or septic thromboembolism, of the portal vein. It most commonly occurs as a complication of diverticulitis or appendicitis and less commonly due to cholecystitis, pancreatitis, and other intra-abdominal infections. Treatment of pylephlebitis with anticoagulation is still controversial due to low occurrence [1]. Plemmons et al. stated that no cases showed clinical improvement with heparin, but that benefit of some anticoagulants could not be ruled out [2]. In this case report, we present a patient who presented with sigmoid diverticulitis that was complicated with pylephlebitis.
Case Report
A 49-year-old Caucasian man was transferred from outside hospital to our ED for increasing weakness, fatigue, nausea, vomiting, and abdominal pain for three weeks and was unable to tolerate oral intake. He had been a daily alcohol user up until three weeks before admission, along with daily marijuana use and presumed his symptoms were due to alcohol withdrawal. Past medical history includes GERD, diverticulitis, and inguinal hernia repair. He did not have colonoscopy due to lack of insurance and financial means. His vitals on presentation were: temperature was 97.1°F, heart rate (HR) elevated at 141 beats/min, respiratory rate (RR) elevated at 28 breaths/min with SpO2 of 98%, and BP low at 102/80 mmHg. On initial evaluation, he appeared toxic, pale, and diaphoretic. Physical exam revealed local peritonitis in the left lower quadrant. Baseline labs were drawn and showed white blood cell (WBC) 26.8 K/uL, hemoglobin 16.6 g/dL, platelet count 89 K/uL, alkaline phosphatase 471 U/L, aspartate transaminase (AST) 271 U/L, alanine transaminase (ALT) 179 U/L, bilirubin 2.5 mg/dL, anion gap 31 mmol/L, and creatinine 2.5 mg/dL. A CT scan showed mild hepatosplenomegaly, proximal sigmoid diverticulitis with gas formation within superior mesenteric vein (SMV) and proximal portal vein.
He was admitted for severe sepsis, dehydration, acute renal failure, transaminitis, and sigmoid diverticulitis with concern for ischemia due to the presence of portal venous gas. Intravenous piperacillin/tazobactam was started. The patient was urgently taken to the operating room for exploratory laparotomy, where he underwent a Hartmann’s procedure, drainage of abscess, and JP drain placement in the pelvis. He received two units of plasma, one unit of platelets, and two units of packed red blood cells (pRBC) intraoperatively and was placed in the intensive care unit (ICU) for postoperative care. He was extubated later that day and blood cultures returned positive for Escherichia coli and Streptococcus species. Pathology of the resected bowel was found to be acute diverticulitis with perforation and abscess. On POD 2, the patient was improving; nasogastric (NG) tube was removed and JP drain had low volume of serosanguineous fluid. Between POD 3 and 5, the patient continued to improve and began having function of his colostomy. On POD 6, the patient had increased abdominal pain and cramping with advancement of diet, but continued to have gas and liquid stool into colostomy bag. On POD 7, the patient’s abdominal pain continued to worsen and large volumes of straw colored fluid began draining from the JP. With acute kidney injury being resolved, a CT abdomen/pelvis with intravenous contrast was obtained and showed thrombosis of SMV, main portal vein, right portal vein, and to less extent left portal vein, which was suggestive of pylephlebitis (Figure 1 and Figure 2). The patient was started on Enoxaparin 1 mg/kg two times a day (BID) with continuation of antibiotics. Due to lack of insurance the patient was transitioned to oral Warfarin. On POD 15, the patient was discharged in stable condition with Levofloxacin 750 mg and Metronidazole 500 mg for an additional four weeks, along with Warfarin 5 mg daily. Upon discharge, the patient had trouble becoming therapeutic on Warfarin presumably due to his liver issues, therefore he was switched to Rivaroxaban after financial resources were obtained. The patient was recommended to remain on Rivaroxaban for a total of six months.

Discussion
Pylephlebitis is a suppurative thrombosis that forms within the portal venous system. It most commonly occurs as a complication of diverticulitis as a result of the inflammatory process [3],[4]. Although the causative relation between pylephlebitis and diverticulitis is high, about 30%, the occurrence of pylephlebitis in general is quite low, about 3% [5],[6]. This occurrence, although low, has increased over the years due to advances in imaging modality [6],[7]. While the incidence rates of pylephlebitis has increased over the years, the mortality rate has dropped. With the increased use of antibiotics and improved imaging modalities, mortality rates dropped to 25% after 1990 [1],[5],[6].
Pylephlebitis usually begins within the small veins that are closely associated with the area of inflammation. The most common route of extension of the thrombosis is the superior mesenteric vein [7]. Due to the fact that pylephlebitis can present with nonspecific symptoms, such as abdominal pain and vomiting, imaging is crucial in diagnosis [8]. The most precise imaging technique to diagnosis pylephlebitis is a CT with oral and IV contrast. This will allow the identification of thrombosis and its extent [7]. If CT with contrast is unavailable due to cost or renal impairment, ultrasound with Doppler flow can be used [5]. A fatal sign that can be seen on CT is the presence of gas [3],[8]. As an indicator of thrombosis, the gas can be present within the portal vein or the branches that form it [8],[9].
The most important factors in treating pylephlebitis are early diagnosis and prompt treatment. The mainstay treatment is broad spectrum antibiotics with controversial discussions on the adjunct of anticoagulation [5],[6]. Although broad spectrum antibiotics will cover the vast majority of potential organisms, the most common causative organism is Bacteriodes fragilis [6],[7]. Antibiotic regimens can include metronidazole, third generation cephalosporins or fluoroquinolones for 4–6 weeks [6],[7]. Additional therapy with anticoagulants is controversial due to the fact that there are reports of resolution with and without [5]. The purpose of anticoagulation is to prevent thrombus extension that could potentially lead to intestinal ischemia. The use of anticoagulants has shown to lower the mortality rates in patients with pylephlebitis and is now becoming a first line therapy [5],[6],[8].
Conclusion
Although rare, pylephlebitis is most commonly diagnosed following diverticulitis. Preoperative portal venous gas could potentially be an early indicator of pylephlebitis. In our case, the diagnosis of pylephlebitis came postoperatively when the patient’s renal function returned to normal and was able to undergo a CT scan with IV contrast. Perhaps if we had received the patient initially and had been able to aggressively resuscitate the patient, we could have obtained an initial CT with IV contrast. If this had been possible, with only localized peritonitis and clinical signs of sepsis, nonoperative management could have been trialed, such as IV antibiotics and IV anticoagulants. Although the role of systemic anticoagulation is unclear in present literature, in our case it certainly improved the patient’s clinical condition.
REFERENCES
1.
Falkowski AL, Cathomas G, Zerz A, Rasch H, Tarr PE. Pylephlebitis of a variant mesenteric vein complicating sigmoid diverticulitis. J Radiol Case Rep 2014;8(2):37–45. [CrossRef]
[Pubmed]

2.
Plemmons RM, Dooley DP, Longfield RN. Septic thrombophlebitis of the portal vein (pylephlebitis): Diagnosis and management in the modern era. Clin Infect Dis 1995;21(5):1114–20. [CrossRef]
[Pubmed]
3.
Häner C, Inderbitzi R, Badulescu M, Teuscher J. Septic pylephlebitis with detection of gas in the portal vein: A rare complication of sigmoid diverticulitis. [Article in German]. Schweiz Med Wochenschr 1998:128(36):1339–44.
[Pubmed]
4.
Yazgan C, Akkas M, Ozmen MM. Inferior mesenteric vein pylephlebitis due to sigmoid diverticulitis. BMJ Case Rep 2015;2015. pii: bcr2015212599. [CrossRef]
[Pubmed]
5.
Kanellopoulou T, Alexopoulou A, Theodossiades G, Koskinas J, Archimandritis AJ. Pylephlebitis: An overview of non-cirrhotic cases and factors related to outcome. Scand J Infect Dis 2010;42(11–12):804–11. [CrossRef]
[Pubmed]
6.
Mendoza Moreno F, Santos Rodriguez A, Díez Gago MR, et al. Pylephlebitis: An uncommon complication of a sigmoid diverticulitis. EC Gastroenterology and Digestive System 2018:5(5):337–41.
7.
Garrett A, Carnish E, Das N, Slome M, Measley R. Once universally fatal: Pylephlebitis. Am J Med 2014;127(7):595–7. [CrossRef]
[Pubmed]
8.
Nobili C, Uggeri F, Romano F, et al. Pylephlebitis and mesenteric thrombophlebitis in sigmoid diverticulitis: Medical approach, delayed surgery. Dig Liver Dis 2007;39(12):1088–90. [CrossRef]
[Pubmed]
9.
Sellner F, Sobhian B, Baur M, et al. Intermittent hepatic portal vein gas complicating diverticulitis—a case report and literature review. Int J Colorectal Dis 2007;22(11):1395–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Heather Cirotta - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asha Shah - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AcknowledgmentsWe are grateful to MidMichigan Hospital System for supporting this project.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Heather Cirotta et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}