 |
Case Report
Accidental prank leading to pneumatic colon injury: A case report
1 MS, FRCS, Senior Consultant Surgeon, Sooriya Hospital, Saligramam, Chennai, India
2 MS, DNB, MNAMS, FAIS, FACS, FRCS (Glasgow), Specialist Surgery, CAPFs Composite Hospital BSF Kadamtala, Siliguri, West Bengal, India
Address correspondence to:
Kaushik Bhattacharya
G616, Uttorayon, Matigara, Siliguri, Postal Code 734010, West Bengal,
India
Message to Corresponding Author
Article ID: 100077Z12TG2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gopalan TR, Bhattacharya K. Accidental prank leading to pneumatic colon injury: A case report. J Case Rep Images Surg 2020;6:100077Z12TG2020.ABSTRACT
Introduction: A case report of an accidental prank leading to a life-threatening pneumatic caecal injury is being reported.
Case Report: A 20-year-old male patient was brought to the emergency with severe pneumoperitoneum and in shock. Emergent exploratory laparotomy after resuscitation revealed caecal perforation. Right hemicolectomy was done and the patient was discharged in a stable condition.
Conclusion: Urgent laparotomy is the essence in saving the life in pneumatic colonic injuries.
Keywords: Barotrauma, Perforation, Pneumoperitoneum
Introduction
Accidental or cruel perverted jokes played by friends or acquaintances can result in a high-pressure air jet column which overcomes the anal sphincter barrier, pushing enormous amounts of air through the anus into the bowel, resulting in colonic perforation with pneumoperitoneum. An urgent laparotomy might be the only option available to save the life of the patient.
Case Report
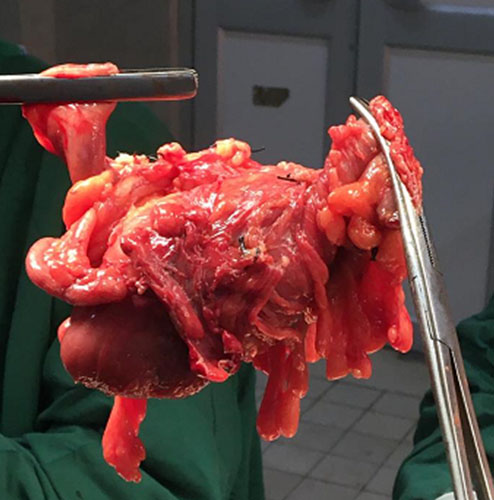
A 20-year-old male patient was brought to the Emergency Department in a collapsed condition. He was barely able to speak or give any type of intelligible history. He had thready feeble pulse of 130/min, gasping for breath and cyanotic, blood pressure (BP) was 70/50 mmHg and respiratory rate was 40/min. His abdomen was tense and distended. History from an attender revealed a prank of inserting a pneumatic cuff of an automobile tire into his anus and inflating it. Immediate resuscitative measures were initiated with intravenous fluids and Foley’s catheterization. An emergent bed side X-ray chest revealed pneumoperitoneum. The patient was immediately shifted for exploratory laparotomy (Figure 1). There was no anal or perineal injury externally. On table, a lacerated caecum and contused proximal ascending colon with minimal soiling in the right paracolic gutter was found. In view of limited localized contamination, decision was taken to avoid any diversion and go for limited resected and anastomosis of the perforated colon. After a thorough peritoneal toileting, a limited right hemicolectomy with Ileoascending anastomosis was done. End to end two layer anastomosis was done with polyglactin 910 and mersilk (Figure 2). The difference in caliber during the anastomosis between ileum and transverse colon was adjusted with a bit of cheating. There was no surgical emphysema or pneumo-mesentery. Resected specimen was sent for histopathology examination. Postoperative course was uneventful, and the patient was started on oral diet on the 4th postoperative day and discharged on the 10th postoperative day in a stable condition. The histopathology report came as caecum showing congestion and areas of hemorrhage consistent with traumatic caecal perforation.

Discussion
Colonic barotrauma due to compressed air may happen because of perversion or accidental injury in industrial zones. Dozens of pneumatic colon injury cases have been reported since the first report by Stone in 1904 [1]. According to the law of Laplace where the tension in the wall is proportional to the radius of the lumen, the risk of iatrogenic barotrauma occurs mostly in caecum due its largest diameter in the entire colon [2]. Injuries may vary from “cat scratch” colon in mild types of iatrogenic barotrauma to colorectal perforation or blowout in the severe variety. It has been seen that the normal colon can withstand a considerable high intraluminal pressure before getting ruptured and the sequence is, when pressure progressively increases, serosal tear occurs first, followed by the muscle and the mucosa in the end. The human colon bursts with only about 120–200 mmHg of pressure and that seromuscular rupture occurs at lower levels [3]. According to the various colonoscopy studies the intraluminal pressure required to perforate the colon was greater than 0.109 kg/cm2 (1.547 psi/80 mmHg) [4]. The patient may develop respiratory distress and hemodynamic instability due to tension pneumoperitoneum. The surgeon should prepare himself to relieve the tension pneumoperitoneum percutaneously with a Veress needle or a cannula. Elevation of the diaphragm due to pressure from below decreases the lung volume affecting ventilation [5]. It is particularly important for the surgeon to immediately prepare himself and his team for urgent laparotomy. Timely intervention is required in such cases to save the life of the victim. Management lies in converting a tension pneumoperitoneum into an open pneumoperitoneum akin to tension pneumothorax. The decision for urgent exploratory laparotomy is a must to decrease the mortality after pneumatic colon injury. The overall mortality of pneumatic rupture of the bowel was 65% and if the patient survives the initial shock, surgical intervention reduced mortality to 42%.
Conclusion
In a case of barotrauma, time is the most important factor in saving the life of a patient. In view of the critical condition in which these types of patients are brought to the emergency department, it is important to start immediate resuscitation along with surgical intervention as soon as the tension pneumoperitoneum is diagnosed. Any delay in management may be fatal.
REFERENCES
1.
Stone GW. Rupture of the bowel caused by compressed air. Lancet 1904;2(4221):216–7.

2.
Kozarek RA, Earnest DL, Silverstein ME, Smith RG. Air-pressure-induced colon injury during diagnostic colonoscopy. Gastroenterology 1980;78(1):7–14.
[Pubmed]
3.
Kozarek RA, Sanowski RA. Use of pressure release valve to prevent colonic injury during colonoscopy. Gastrointest Endosc 1980;26(4):139–42. [CrossRef]
[Pubmed]
4.
Sy ED, Chiu YI, Shan YS, Ong RL. Pneumatic colon injury following high pressure blow gun dust cleaner spray to the perineum. Int J Surg Case Rep 2015;6C:218–21. [CrossRef]
[Pubmed]
5.
Weber M, Kolbus F, Dressler J, Lessig R. Survived ileocaecal blowout from compressed air. Int J Legal Med 2011;125(2):283–7. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
TR Gopalan - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kaushik Bhattacharya - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 TR Gopalan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}