 |
Case Report
Resection of two successive single lung metastases from rectal cancer: A case report and literature review
1 Resident doctor, Department of Thoracic Surgery, Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, China
2 Attending doctor, Department of Thoracic Surgery, Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, China
3 Chief physician, Department of Thoracic Surgery, Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, China
Address correspondence to:
Shao-nan Xie
Attending doctor, Department of Thoracic Surgery, Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei,
China
Message to Corresponding Author
Article ID: 100093Z12YL2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Liu Yb, Cui Dy, Xie Sn, Liu Qy. Resection of two successive single lung metastases from rectal cancer: A case report and literature review. J Case Rep Images Surg 2021;7:100093Z12YL2021.ABSTRACT
Introduction: After the liver, lung is the next most common metastases site of rectal cancer. But the surgical treatment of lung metastases in colorectal cancer (CRC) patients is still controversial.
Case Report: Here we report a 36-year-old male patient who survived 48 months without tumor after radical resection of colorectal cancer, 24 months without tumor after lung metastasis and surgical resection, and 42 months without tumor after recurrence of metastasis and surgical resection.
Conclusion: Surgical resection of solitary pulmonary metastases in CRC patients can benefit patients.
Keywords: Colorectal cancer, Lung metastases, Surgical treatment
Introduction
After the liver, lung is the next most common metastases site of rectal cancer [1]. In the past, it was considered that distant organ recurrence and metastasis were the contraindication of surgery. However, after long-term clinical practice, some consensus has been reached on the indications of surgical resection of rectal cancer and lung metastases. Although one study supports that surgical resection of lung metastases can improve the long-term survival of rectal cancer patients [2], but there are still some scholars who are against it [3]. It has also been reported that the postoperative survival of patients is related to the time interval of occurrence of postoperative metastases, the number of metastases and the resectability of metastases [4].
Case Report
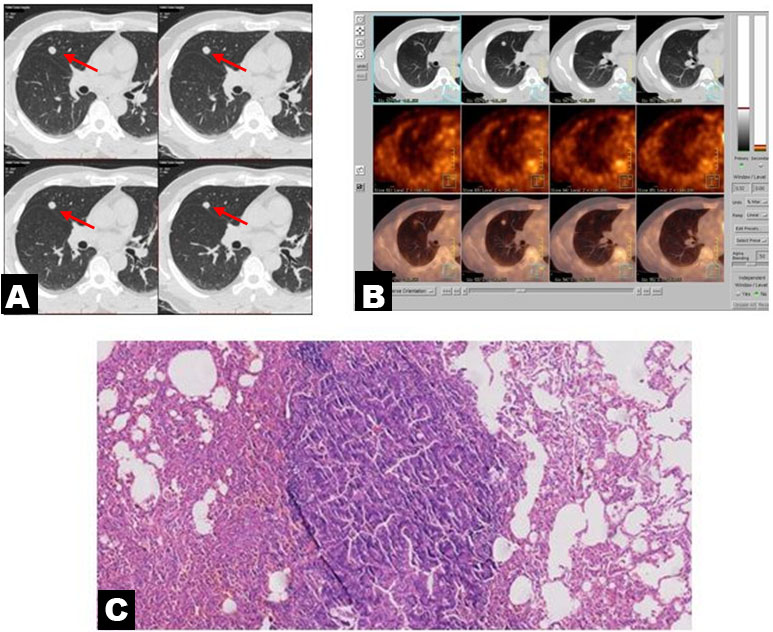
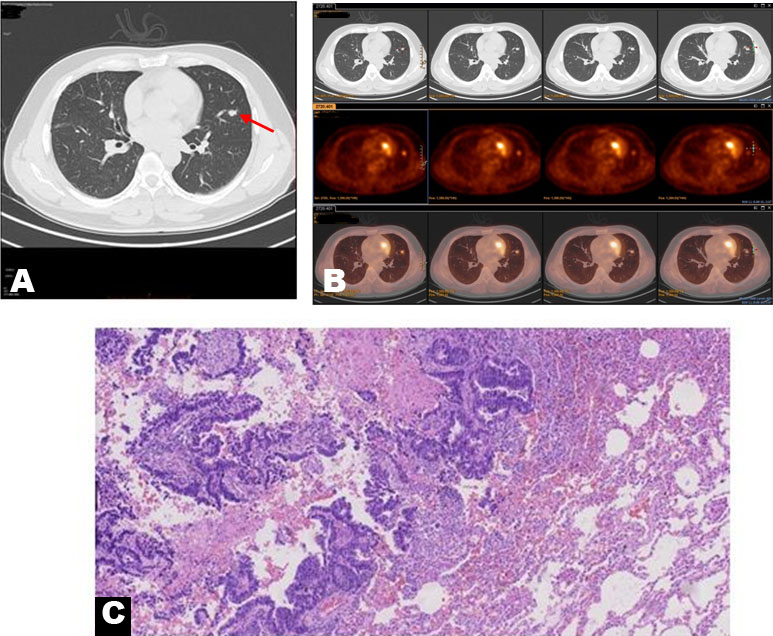
Here we report a case of 36-year-old male patient who was diagnosed with rectal cancer in July 2011 and underwent Miles operation for rectal cancer. The postoperative pathology was “adenocarcinoma invading surrounding soft tissue.” Clinical upper and lower disability (−). 0/3 of the root, 0/5 of the middle, and 1/5 of the para intestinal lymph nodes metastasized. The postoperative pathological stage was stage IIIB (T4aN1M0). FOLFOX regimen was used as adjuvant chemotherapy for 6 cycles. In July 2015, according to the follow-up plan, the right upper lobe nodule was found (Figure 1A), positron emission tomography/computed tomography (PET/CT) showed abnormal hypermetabolism with a maximum standard uptake value (SUV) of 4.0 (Figure 1B), no abnormality was found in the rest cases, which was considered as postoperative lung oligometastasis of rectal cancer. The right upper lobe tumor was wedge-shaped resected by video-assisted thoracoscopy and the surrounding lymph nodes were sampled. The postoperative pathology was “adenocarcinoma of digestive tract origin,” and no clear invasion of visceral pleura was found. Lymph nodes: 4 group 0/2, 7 group 0/3, 8 group 0/1, 9 group 0/1, 10 group 0/2, 11 group 0/1 (Figure 1C). FOLFOX regimen was given for 4 cycles after operation, and then followed up regularly. In July 2017, the left upper lobe lingual nodule was found (Figure 2A), PET/CT showed that the left upper lobe nodule was new, with abnormal hypermetabolism, and the maximum SUV was 2.5 (Figure 2B). The pulmonary oligarchy metastasis was considered. The pathological results were: gastrointestinal adenocarcinoma, lymph node: 7 group 0/1, 5 group 0/1, 6 group 0/1, 10 groups 0/2 metastasis (Figure 2C). FOLFIRI regimen was used for 6 cycles. Up to January 2021, the patient was still tumor free.
Discussion
According to the data of GLOBOCAN 2018, the global incidence of CRC ranks fourth (6.1%) of all cancers, and the mortality rate (9.2%) ranks second [5]. There is a 5% risk of colorectal cancer in one’s life, although this number may decrease with the development of early diagnosis and treatment of colorectal cancer [6]. The 5-year overall survival rate of CRC patients is about 65%, which is closely related to the clinical stage of patients [7]. Although great progress has been made in the diagnosis and treatment of CRC [8],[9],[10],[11], but so far, there are still many colon cancer patients with distant metastasis and recurrence in the course of treatment. How to effectively improve the treatment effect of colorectal cancer, so that patients get better long-term survival is still a difficult task [12].
Lung is the most easily metastasized organ of colorectal cancer. About 20% of colorectal cancer patients have seen lung metastasis at the first visit. About 10% of patients who have undergone radical colorectal cancer resection will still have long-term lung metastasis, most of which are accompanied by other organs metastasis of the whole body, and the opportunity of operation will be lost [13],[14]. However, 2–4% of all patients with lung metastases from colorectal cancer are localized lung metastases. Can surgical resection of lung metastases improve the long-term survival rate of these patients? It has been reported that the 5-year survival rate of CRC patients with localized lung metastasis after operation is 21–64%, which is similar to that of CRC patients with localized liver metastasis after operation [15]. Since the first case of colorectal cancer lung metastasis surgery, although there is no randomized controlled study, most of the related articles are from the registration data, retrospective analysis and case analysis, but the benefits of surgery are still widely accepted [16]. Moreover, multiple resection of lung metastases can still improve the prognosis, so surgical treatment is recommended for this kind of patients. The treatment of lung metastases has become an integral part of the comprehensive treatment of colorectal cancer. Selective surgical resection can prolong the life of patients [17].
It can be seen that in the previous retrospective analysis, surgical resection is preferred for colorectal cancer with lung metastasis. Due to uncertain factors such as difficult recruitment and rapid progress of patients with lung metastasis from colorectal cancer, many trials were terminated because they could not reach the expected statistical endpoint. Pulmonary metastasectomy versus continued active monitoring in colorectal cancer (PulMiCC) trial is the only ongoing prospective clinical study of colorectal cancer with lung metastases. The purpose of this study is to compare the clinical effects of active monitoring and resection and active monitoring of lung metastases. The latest research results show that, for patients with lung metastasis of colorectal cancer, lung metastasis resection has no survival benefit, which indicates that lung metastasis resection may not improve the survival rate of patients with lung metastasis of colorectal cancer [18]. Tom Treasure believes that for patients with colorectal cancer, lung metastasis resection is unlikely to bring significant survival benefits, nor can it alleviate the patient’s condition. Moreover, whether it is surgery or radiofrequency ablation, there are risks and increase the cost of treatment [19].
Chemotherapy combined with immunotherapy or targeted therapy cannot get satisfactory therapeutic effect. One study points out that pulmonary colorectal metastases treated with stereotactic body radiation therapy have a higher risk of local recurrence than those treated with wedge resection [20]. For CRC patients with postoperative lung metastasis, we cannot completely abandon lung metastasis resection because of PulMiCC research results. After careful study of PulMiCC study, we found that among the 65 patients enrolled in PulMiCC study, 17 patients had previous liver metastasis resection [18]. These results indicate that CRC patients with lung metastasis have multiple distant metastasis of colorectal cancer, rather than CRC patients with few lung metastasis. Without strict preoperative screening, patients with poor prognosis were enrolled. It has been reported that the recurrence rate of CRC patients with lung metastasis after the first pneumonectomy is more than 50% [21]. However, repeated resection of lung metastases is a safe treatment for patients who have undergone rigorous preoperative evaluation [22]. Our case report also confirmed these conclusions. The patient had two successive single lung metastases after rectal cancer surgery. After resection, the patient still survived without tumor and has achieved long-term survival.
According to National Comprehensive Cancer Network (NCCN) guidelines, surgical indications for lung metastases from colon cancer include [23]: (1) if sufficient lung function is reserved, complete resection shall be carried out according to the anatomical location and scope of invasion of the metastasis; (2) the primary tumor has been completely removed; (3) the presence of resectable extrapulmonary metastasis is not a taboo; (4) if the cases meet certain conditions, it is feasible to resect them again. Lung metastasis of colorectal cancer can be single, multiple, single lung, or bilateral lung. The principle of surgical treatment is to resect tumor tissue to the maximum extent, to keep the normal lung tissue function to the maximum extent, and to guarantee the quality of life of patients after operation. The surgical method is to select partial lung resection (wedge-shaped resection and segmental resection), while lobectomy and compound lobectomy should be careful to avoid total lung resection, so as to provide another or multiple operation opportunities for the recurrence of lung metastasis in the future. Wedge resection 0.5–1 cm away from the focus is a classic operation for peripheral lung lesions [24]. David B. Nelson pointed out that in surgical resection of colorectal lung metastasis, the risk of local recurrence is related to the length of resection margin and tumor size. However, as long as there is enough edge length, the increased risk of local recurrence due to larger tumors can be reduced [25]. Segmental resection can be performed for local multiple metastases and lobectomy can be performed for recurrent or multiple metastases. At the same time, we need to consider the patient’s general condition, tolerance to surgery, and other factors. With the improvement of thin-layer high-resolution CT scanning and PET scanning, the sensitivity of preoperative examination has been greatly improved. Many researchers support that thoracoscopic surgery has the same therapeutic effect as thoracotomy. They believe that thoracoscopic surgery can obtain the same 5-year survival rate and reduce the incidence of postoperative complications. For multiple or suspected multiple pulmonary metastases or pulmonary metastases near the pulmonary hilar vessels, we recommend thoracotomy for resection, so that surgeons can palpate the metastases not found by imaging examination, avoid missing small lesions, facilitate the treatment of vascular bronchus, and retain as much normal lung tissue as possible.
Although there is no unified standard for the scope of thoracic lymph node dissection in colorectal cancer patients with lung metastases, a large number of literatures show that the lymph node status of patients with lung metastases has a great impact on the prognosis. Ercan reported that the 3-year survival rate of patients with negative lymph nodes was 69%, and that of patients with positive lymph nodes decreased to 38%; the 5-year survival rate of patients with complete resection of lung metastases was 30–50%, but that of patients with lymph node involvement was less than 20% [26]. In 167 patients with colorectal lung metastasis who underwent systematic lymph node dissection, 16 cases were found to have lymph node metastasis between hilar or lobular fissure, and 16 cases were found to have mediastinal lymph node metastasis [27]. To summarize the number and size of lung metastasis increased the risk of mediastinal lymph node involvement, and the location of the lymph nodes affected the long-term survival of patients, it is recommended that if extensive mediastinal lymph nodes are suspected of involvement before operation, the resection of pulmonary metastasis should be delayed. It is important to note that those imaging suspected metastasis lymph nodes may be proved to be false positive by surgery. Although lymph node metastasis is very important for predicting prognosis, no surgeon believes that routine systematic lymph node dissection can improve the prognosis of patients with colorectal cancer with lung metastasis. In the existing colorectal cancer patients with lung metastasis, lymph node cleaning or sampling is not routine, and the treatment of lymph nodes needs further study.
So far, there are still some controversies about the surgical treatment of lung metastasis in CRC patients. Because of the short follow-up time of patients with pulmonary metastasis, less patients in the group and the heterogeneity of lung metastasis, there are no relevant large sample clinical control test results, so there is still a dispute about the surgical treatment of lung metastasis. We report that this patient has been free of tumor after radical resection of colorectal cancer for 48 months, and has had lung metastasis and has no tumor after resection for 24 months. It has been 42 months since the tumor was removed and the tumor free after surgery.
Conclusion
Therefore, surgical resection of solitary pulmonary metastases in CRC patients can benefit patients. The patients with lung metastasis with long interval without tumor, low malignant degree of primary tumor, no metastasis of other organs, and the patients with metastasis who can be completely removed may benefit most from the lung metastasis resection. Therefore, if the patients with colorectal cancer lung metastasis want to undergo lung metastasis resection, they should more strictly select the patients’ indications, so as to achieve good treatment effect.
REFERENCES
1.
Treasure T, MiloševićM, Fiorentino F, Macbeth F. Pulmonary metastasectomy: What is the practice and where is the evidence for effectiveness? Thorax 2014;69(10):946–9. [CrossRef]
[Pubmed]

2.
Davini F, Ricciardi S, Zirafa CC, et al. Lung metastasectomy after colorectal cancer: Prognostic impact of resection margin on long term survival, a retrospective cohort study. Int J Colorectal Dis 2020;35(1):9–18. [CrossRef]
[Pubmed]
3.
Van Raemdonck D, Treasure T, Van Cutsem E, Macbeth F. Pulmonary metastasectomy in colorectal cancer: Has the randomized controlled trial brought enough reliable evidence to convince believers in metastasectomy to reconsider their oncological practice? Eur J Cardiothorac Surg 2021;59(3):517–21. [CrossRef]
[Pubmed]
4.
Pastorino U, Buyse M, Friedel G, et al. Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. J Thorac Cardiovasc Surg 1997;113(1):37–49. [CrossRef]
[Pubmed]
5.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68(6):394–424. [CrossRef]
[Pubmed]
6.
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin 2021;71(1):7–33. [CrossRef]
[Pubmed]
7.
Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin 2020;70(3):145–64. [CrossRef]
[Pubmed]
8.
Brachet Contul R, Grivon M, Fabozzi M, et al. Laparoscopic total mesorectal excision for extraperitoneal rectal cancer: Long-term results of a 18-year single-centre experience. J Gastrointest Surg 2014;18(4):796–807. [CrossRef]
[Pubmed]
9.
Cui YM, Jiang D, Zhang SH, et al. FOXC2 promotes colorectal cancer proliferation through inhibition of FOXO3a and activation of MAPK and AKT signaling pathways. Cancer Lett 2014;353(1):87–94. [CrossRef]
[Pubmed]
10.
Dvorak HF. Tumor stroma, tumor blood vessels, and antiangiogenesis therapy. Cancer J 2015;21(4):237–43.
[Pubmed]
11.
Abrahao ABK, Ko YJ, Berry S, Chan KKW. A comparison of regorafenib and tas-102 for metastatic colorectal cancer: A systematic review and network meta-analysis. Clin Colorectal Cancer 2018;17(2):113–20. [CrossRef]
[Pubmed]
12.
National Health Commission of the People’s Republic of China. Chinese protocol of diagnosis and treatment of colorectal cancer (2020 edition). [Article in Chinese]. Zhonghua Wai Ke Za Zhi 2020;58(8):561–85. [CrossRef]
[Pubmed]
13.
Goya T, Miyazawa N, Kondo H, Tsuchiya R, Naruke T, Suemasu K. Surgical resection of pulmonary metastases from colorectal cancer. 10-year follow-up. Cancer 1989;64(7):1418–21.
[Pubmed]
14.
McCormack PM, Burt ME, Bains MS, Martini N, Rusch VW, Ginsberg RJ. Lung resection for colorectal metastases. 10-year results. Arch Surg 1992;127(12):1403–6. [CrossRef]
[Pubmed]
15.
Sternberg DI, Sonett JR. Surgical therapy of lung metastases. Semin Oncol 2007;34(3):186–96. [CrossRef]
[Pubmed]
16.
Nichols FC. Pulmonary metastasectomy: Role of pulmonary metastasectomy and type of surgery. Curr Treat Options Oncol 2014;15(3):465–75. [CrossRef]
[Pubmed]
17.
Kim HJ, Kye BH, Lee JI, et al. Surgical resection for lung metastases from colorectal cancer. J Korean Soc Coloproctol 2010;26(5):354–8. [CrossRef]
[Pubmed]
18.
Treasure T, Farewell V, Macbeth F, et al. Pulmonary Metastasectomy versus Continued Active Monitoring in Colorectal Cancer (PulMiCC): A multicentre randomised clinical trial. Trials 2019;20(1):718. [CrossRef]
[Pubmed]
19.
Treasure T, Macbeth F, Farewell V, Williams NR, Fallowfield L. The fallacy of large survival gains from lung metastasectomy in colorectal cancer. Lancet 2021;397(10269):97–8. [CrossRef]
[Pubmed]
20.
Nelson DB, Tayob N, Nguyen QN, et al. Local failure after stereotactic body radiation therapy or wedge resection for colorectal pulmonary metastases. J Thorac Cardiovasc Surg 2019;158(4):1234–41.e16. [CrossRef]
[Pubmed]
21.
Gonzalez M, Ris HB, Krueger T, Gervaz P. Colorectal cancer and thoracic surgeons: Close encounters of the third kind. Expert Rev Anticancer Ther 2012;12(4):495–503. [CrossRef]
[Pubmed]
22.
Zellweger M, Abdelnour-Berchtold E, Krueger T, Ris HB, Perentes JY, Gonzalez M. Surgical treatment of pulmonary metastasis in colorectal cancer patients: Current practice and results. Crit Rev Oncol Hematol 2018;127:105–16. [CrossRef]
[Pubmed]
23.
Warwick R, Page R. Resection of pulmonary metastases from colorectal carcinoma. Eur J Surg Oncol 2007;33 Suppl 2:S59–63. [CrossRef]
[Pubmed]
24.
Pfannschmidt J, Muley T, Hoffmann H, Dienemann H. Prognostic factors and survival after complete resection of pulmonary metastases from colorectal carcinoma: Experiences in 167 patients. J Thorac Cardiovasc Surg 2003;126(3):732–9. [CrossRef]
[Pubmed]
25.
Nelson DB, Tayob N, Mitchell KG, et al. Surgical margins and risk of local recurrence after wedge resection of colorectal pulmonary metastases. J Thorac Cardiovasc Surg 2019;157(4):1648–55. [CrossRef]
[Pubmed]
26.
Ercan S, Nichols FC 3rd, Trastek VF, et al. Prognostic significance of lymph node metastasis found during pulmonary metastasectomy for extrapulmonary carcinoma. Ann Thorac Surg 2004;77(5):1786–91. [CrossRef]
[Pubmed]
27.
Pfannschmidt J, Klode J, Muley T, Dienemann H, Hoffmann H. Nodal involvement at the time of pulmonary metastasectomy: Experiences in 245 patients. Ann Thorac Surg 2006;81(2):448–54. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Yong bin Liu - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dong-yu Cui - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shao-nan Xie - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Qing-yi Liu - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Yong-bin Liu et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}