 |
Case Report
Periodontal disease as a cause of intraperitoneal mesh infection: A case report
1 MBBS, General Surgical Principal House Officer, Cairns Base Hospital, Cairns, Australia
2 MBBS, FRACS, Staff Specialist - General Surgeon, Cairns Base Hospital, Cairns, Australia
Address correspondence to:
Ken Hoc Lam
Cairns Base Hospital, Cairns,
Australia
Message to Corresponding Author
Article ID: 100097Z12KL2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Lam KH, Brunott N. Periodontal disease as a cause of intraperitoneal mesh infection: A case report. J Case Rep Images Surg 2021;7:100097Z12KL2021.ABSTRACT
This case report describes a delayed intraperitoneal mesh infection suspected to be a result of hematogenous spread from periodontal disease. A 46-year-old gentleman presented to the emergency department with a 2-week history of worsening periumbilical pain, erythema, and purulent discharge on the background of having an intraperitoneal Bard Ventralex mesh [composite polypropylene/expanded polytetrafluoroethylene (ePTFE)] placed as part of an emergent open primary umbilical hernia repair four years prior. Contrast-enhanced computed tomography (CT) of the abdomen confirmed mesh involvement. He proceeded to laparoscopic exploration revealing an abscess cavity between the anterior abdominal wall and the mesh requiring mesh explantation. The mesh cultured Prevotella intermedia—a gram negative anaerobe associated with periodontitis. This case report suggests that mesh can be colonized with bacteria from the oral cavity resulting in clinically significant infection.
Keywords: Case report, Intraperitoneal mesh infection, Periodontal disease, Prevotella intermedia
Introduction
Mesh placement is part of the standard approach to ventral hernia repair due to a significant reduction in recurrence rate [1]. Bacterial colonization of the mesh can result in biofilm formation and infection can be difficult to manage [1]. Postoperative infection usually presents within three months of the initial operation although late-onset infection has also been described [2]. Recognized mechanisms of mesh infection include intraoperative contamination during placement, contamination of the mesh from a subsequent procedure, and spread to the mesh from the skin or gastrointestinal tract [3],[4],[5],[6]. We present the case of a 46-year-old man who presented four years after his index operation with intraperitoneal mesh infection which cultured Prevotella intermedia. We propose that this episode of mesh infection may relate to hematogenous spread as a result of transient bacteremia from periodontal disease representing a mechanism not well described in the literature.
Case Report
Mr. PD (46) presented to the emergency department with a 2-week history of umbilical pain, erythema, and purulent discharge. His background was significant for an emergent open repair of an incarcerated umbilical hernia containing omental fat four years prior. Routine antibiotic prophylaxis was administered, and an 8 cm Bard ventral patch [composite polypropylene/expanded polytetrafluoroethylene (ePTFE)] was placed in the intraperitoneal position.
His vital signs were within normal limits. Clinical examination revealed a 5 cm area of erythema and active purulent discharge at the site of the previous umbilical repair. Biochemical evaluation revealed a white cell count of 13.9×109/L (reference range 4–11×109/L) with neutrophilia and an elevated c-reactive protein (CRP) of 49 mg/L (reference range <5.0 mg/L). A contrast-enhanced computed tomography (CT) of the abdomen was suggestive of mesh involvement (Figure 1).
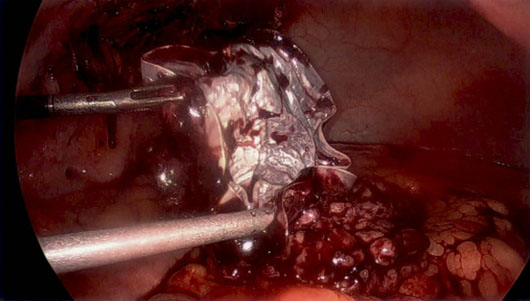
He was treated with empiric intravenous (IV) Flucloxacillin, analgesia, and fluid resuscitation with the view to laparoscopic mesh explantation. Intraoperatively, he was found to have omentum adherent to the posterior side of the mesh. An infected pocket of pus was found between the abdominal wall and the polypropylene layer of the mesh anteriorly. The mesh was explanted with lap scissor diathermy and sent for culture (Figure 2). The abdominal wall remained intact and there was no resultant defect to repair. The affected area was washed and suctioned and a 15Fr drain was placed. The mesh culture isolated P. intermedia—an organism commonly associated with poor dentition. The patient’s antibiotic cover was broadened to Amoxicillin with Clavulanic acid. The patient continued to have five further days of IV antibiotics and had an otherwise uneventful recovery and was discharged with oral antibiotics.
The infectious diseases team was consulted, and an oral exam and orthopantomogram showed no dental abscess. He was subsequently seen in clinic one week later with complete resolution of his abdominal symptoms but was complaining of right sided tooth pain with mastication for which he was referred to the dentist. He has not responded to further attempts at follow-up.

Discussion
Mesh placement is widely used to reduce recurrence risk in umbilical hernia repair [1]. Depending on the type of mesh, infection can occasionally be managed with percutaneous drainage, irrigation, and antibiotics alone in an attempt to salvage the mesh but failure of this necessitates operative removal [7],[8]. The incidence of mesh infection after an open hernia repair is up to 10.2% and most commonly occurs within three months of the operation [3],[5]. While there are reports of delayed mesh infection it is highly unusual for a patient to present four years after their index operation. Established risk factors for developing mesh infection include active smoking, American Society of Anaesthesiologists score (ASA) ≥3, and advanced age [4]. Other factors including defect size, length of operation and operator experience, technique of repair and placement of mesh, and type of mesh used would likely have an impact although the data supporting this is inconsistent [4]. Apart from active smoking, this patient did not have any of the other established risk factors.
A small study by Cobb et al. suggested that Staphylococcus aureus was the most common organism grown in cases of infected mesh implying operative contamination although other species of Staphylococcus and Streptococcus as well as anaerobes have been described [3].
Langbach et al. used rRNA to characterize the microbiome of mesh samples from 30 patients requiring recurrent ventral hernia repair who did not have clinical signs of infection and found that typical oral bacteria were more commonly found colonizing mesh as compared to skin and enteric organisms. More interestingly these bacteria matched those of samples collected from patients with periodontal disease [9]. A review of the literature has not previously described P. intermedia as a source of intra-abdominal mesh infection. Prevotella intermedia is a gram negative anaerobe usually associated with periodontal disease but has also been described as a pathogen related to infectious aortitis [10],[11].
Possible contamination sources may include a failure of sterilization or aseptic technique, or contamination of the mesh from a subsequent procedure such as seroma drainage or a separate abdominal operation. However, this patient did not have any subsequent procedures which could have resulted in mesh colonization. Skin and gut sources are possible sources of mesh infection but not a usual source of P. intermedia.
Conclusion
We propose that this episode of mesh infection is most likely due to hematogenous spread from periodontal disease given the very late onset of his infection, patient clinical findings, and isolation of P. intermedia—a bacterium strongly associated with poor dentition. Treatment options range from conservative management with intravenous antibiotics to mesh explantation—a modality that was preferred in this situation with complete resolution of symptoms.
REFERENCES
1.
Earle D, Roth JS, Saber A, et al. SAGES guidelines for laparoscopic ventral hernia repair. Surg Endosc 2016;30(8):3163–83. [CrossRef]
[Pubmed]

2.
Chen T, Zhang YH, Wang HL, Chen W, Wang J. Late-onset deep mesh infection: A study of eight cases detected from 2666 consecutive patients with abdominal wall hernia repairs. Chin Med J (Engl) 2016;129(15):1870–2. [CrossRef]
[Pubmed]
3.
Cobb WS, Carbonell AM, Kalbaugh CL, Jones Y, Lokey JS. Infection risk of open placement of intraperitoneal composite mesh. Am Surg 2009;75(9):762–8.
[Pubmed]
4.
Mavros MN, Athanasiou S, Alexiou VG, Mitsikostas PK, Peppas G, Falagas ME. Risk factors for mesh-related infections after hernia repair surgery: A meta-analysis of cohort studies. World J Surg 2011;35(11):2389–98. [CrossRef]
[Pubmed]
5.
Petersen S, Henke G, Freitag M, Faulhaber A, Ludwig K. Deep prosthesis infection in incisional hernia repair: Predictive factors and clinical outcome. Eur J Surg 2001;167(6):453–7. [CrossRef]
[Pubmed]
6.
Bliziotis IA, Kasiakou SK, Kapaskelis AM, Falagas ME. Mesh-related infection after hernia repair: Case report of an emerging type of foreign-body related infection. Infection 2006;34(1):46–8. [CrossRef]
[Pubmed]
7.
Aguilar B, Chapital AB, Madura JA 2nd, Harold KL. Conservative management of mesh-site infection in hernia repair. J Laparoendosc Adv Surg Tech A 2010;20(3):249–52. [CrossRef]
[Pubmed]
8.
Shubinets V, Carney MJ, Colen DL, et al. Management of infected mesh after abdominal hernia repair: Systematic review and single-institution experience. Ann Plast Surg 2018;80(2):145–53. [CrossRef]
[Pubmed]
9.
Langbach O, Kristoffersen AK, Abesha-Belay E, Enersen M, Røkke O, Olsen I. Oral, intestinal, and skin bacteria in ventral hernia mesh implants. J Oral Microbiol 2016;8:31854. [CrossRef]
[Pubmed]
10.
Maeda N, Okamoto M, Kondo K, et al. Incidence of prevotella intermedia and Prevotella nigrescens in periodontal health and disease. Microbiol Immunol 1998;42(9):583–9. [CrossRef]
[Pubmed]
11.
Boersma C, Kampschreur LM, Buter H, Doorenbos BM, Klinkert P, Koning GG. Prevotella intermedia infection causing acute and complicated aortitis—A case report. Int J Surg Case Rep 2017;32:58–61. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ken Hoc Lam - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nathan Brunott - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Ken Hoc Lam et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}