 |
Case Report
Huge surgical emphysema and pneumomediastinum as a sequela to conservative dental restoration: A case report
1 MBBS – General Surgical Unaccredited Registrar, Department of General Surgery, Cairns Hospital, North Cairns, Queensland, Australia
2 MBBS – General Surgical Registrar, Department of General Surgery, Cairns Hospital, North Cairns, Queensland, Australia
3 FRACS – General Surgical Consultant, Department of General Surgery, Cairns Hospital, North Cairns, Queensland, Australia
Address correspondence to:
Arun Nadarajah
Department of General Surgery, Cairns Hospital, North Cairns, Queensland,
Australia
Message to Corresponding Author
Article ID: 100099Z12AN2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Nadarajah A, Arron TY, Elston T. Huge surgical emphysema and pneumomediastinum as a sequela to conservative dental restoration: A case report. J Case Rep Images Surg 2022;8(1):1–4.ABSTRACT
Introduction: Subcutaneous emphysema and pneumomediastinum are rare sequelae of dental restorative procedure. Etiology includes tooth extraction, preparation of teeth, dental restoration, endodontic treatment, and subgingival curettage. All of which are related to the use of high-pressure manual and motorized tools.
Case Report: We present a rare case of elaborate pneumomediastinum with subcutaneous emphysema in a 75-year-old man who underwent a single molar “44” dental filling and presented to our regional hospital with the main complaint of facial swelling and odynophagia 1 hour post-procedure. The patient was managed conservatively through an uneventful hospital course, and fully recovered.
Conclusion: This case highlights the need for prompt diagnosis and management of subcutaneous emphysema and pneumomediastinum because of the risk of airway compromise, air embolism, and infection. Awareness of relatively “benign” pneumomediastinum as a result of a dental procedure is important especially in the rural and remote setting among general surgical teams. The mechanism, clinical presentation, differential diagnosis, and complications are also reviewed.
Keywords: Dental filling, Pneumomediastinum, Surgical emphysema
Introduction
Pneumomediastinum and subcutaneous emphysema have an extensive etiology list ranging from infection or trauma to spontaneous origin or even post-operative [1]. It can also be a rare but serious complication of dental and oral surgery procedures [2]. Air being driven underneath the tissue causes the disorder, which can also migrate along the fascial planes to the periorbital, mediastinal, pericardial, and/or thoracic regions, swelling, and crepitus when touched [3]. Subcutaneous emphysema can be caused by several dental treatments such as crown preparations, other operative procedures, endodontic therapy, tooth extractions where osteotomy has been carried out or tooth extractions that have required using burs for dental sectioning. The bulk of case reports seem to link subcutaneous emphysema to the use of air-driven high-speed handpieces; however, perioperative events like endotracheal intubation and positive pressure ventilation have also been documented [4].
Following dental treatments, pressured air drills are frequently to blame for subcutaneous emphysema and pneumomediastinum, which affect the mandibular molars [5].
High-speed air turbine drills are most frequently utilized in dental restoration procedures since they are made for cutting teeth. These drills may be used in exodontia to section teeth and aid tooth extraction, even though specific closed turbine systems are available for oral surgical operations. These air turbine drills, which are currently in general use, are propelled by compressed air rotating at a speed of 450,000 rpm and 3.5–4.0 kgf/cm2. Emphysema has been recorded to develop following dental procedures involving the use of an air turbine specially when soft tissues are not well adhered to the bone. However, few cases have progressed to affect the mediastinum [3],[6]. However, the majority of cases are usually self-limiting and benign [7].
A very typical clinical pathology, subcutaneous cervicofacial emphysema includes a long range of differential diagnoses, such as angioedema and/or allergic reaction, deep neck space infections, necrotizing fasciitis, airway injury, dental or surgical operations, pneumothorax, or pneumomediastinum. By using a clinical history, clinical examination, and the proper radiographic and laboratory testing, iatrogenic subcutaneous emphysema can be identified. The first instance of subcutaneous emphysema is as a result of dental work in 1900 [8].
We report a case of cervical subcutaneous emphysema and pneumomediastinum occurring after extraction of a mandibular right first molar using an air turbine drill. The emphysema was detected a few hours after dental surgery while the patient was eating. It is essential to know that these complications may arise following innocuous dental procedures such as tooth extraction, although they are far more rare but more prevalent in the geriatric population due to the physiological alteration or weakening of connective tissue [9].
The aim of this case report is to bring awareness among rural and remote surgical teams of complications following common procedures (including dental) and be able to readily care for patients.
Case Report
The patient is a 75-year-old man who was referred by his dentist with significant right facial swelling, dysphagia, and odynophagia 4 hours after his dental filling procedure. He had his right lower premolar tooth (tooth 44) filling done under local anesthesia. It was uncomplicated when he first had the procedure. The patient had subsequently noticed right unilateral facial swelling with odynophagia when he was eating 1 hour post-procedure. He denied to have any respiratory distress. His symptoms unfortunately had progressed and hence were referred by a dentist to the emergency department. He had background history of multiple previous dental fillings, benign prostate hypertrophy, and hypercholesterolemia.
On examination, he had normal vital signs. He was alert with no difficulty of breathing and he was able to speak in full sentences. He had obvious swelling over the temporal, right cheek, neck, and upper chest. He had clinical crepitus noted with palpation. In addition, a small tongue bite was seen but no obvious mucosal wound was noted.
His biochemical markers on presentation were unremarkable with normal white cell count, liver function, kidney function as well as C-reactive protein level.
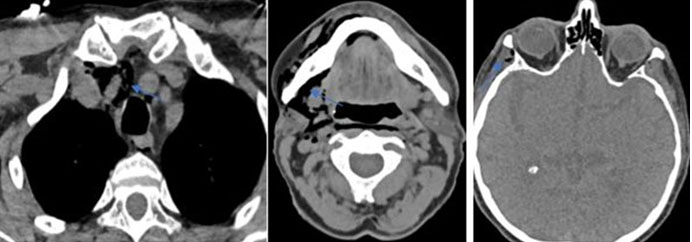
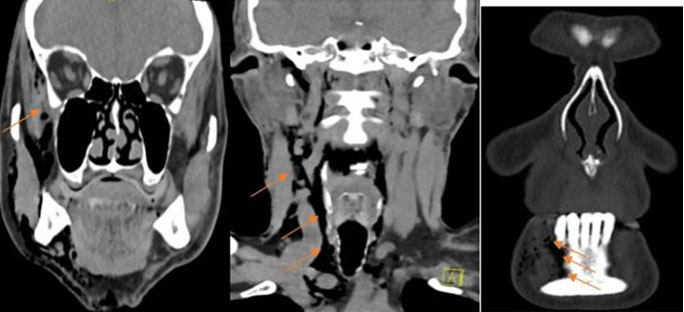
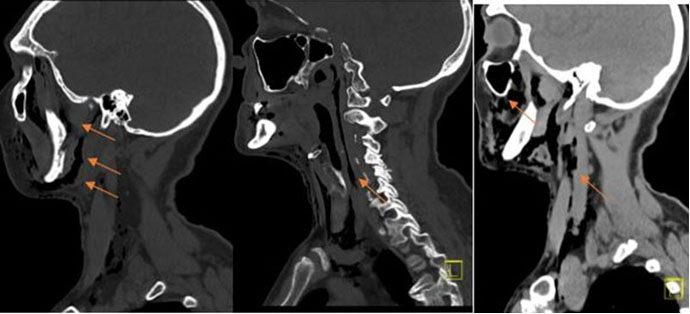
A computed tomography (CT) of head and neck (Figure 1, Figure 2, Figure 3) was conducted and revealed that a significant subcutaneous emphysema overlying the right mid-face extending inferiorly to the level of the angle of mandible, submandibular space, right infratemporal fossa, right parapharyngeal space, lower neck, and superior mediastinum. The bony contours of the maxillary sinuses, parotid, or submandibular gland were all preserved. No evidence of bony injury of the right mandibular body, intraorbital gas, and pneumothorax were identified.
An urgent surgical consult was asked as necrotizing fasciitis was one of the concerns. An urgent maxillofacial review was also requested. It was deemed that Mr. WP’s symptoms were most likely to be caused by pneumatic dental drilling device. He was treated conservatively with intravenous amoxicillin/clavulanic acid 1000 mg/200 mg three times per day and observed in hospital for 24 hours. He was discharged with oral Augmentin duo forte on day 1 admission.
Discussion
Subcutaneous emphysema can be a serious complication of dental or surgical therapy. Although subcutaneous emphysema seldom results in long-term morbidity, prevention of development depends on early detection and appropriate care. When air is pressed into the fascial gaps of the tissue, subcutaneous emphysema develops. Dissection is possible along the relatively fragile connective tissue connecting adjacent muscle planes once the air is under the tissue. Air from the mandibular region can spread to the retropharynx, mediastinal, pericardial, or thoracic spaces thanks to the communication of the fascial spaces. Additionally, the patient’s coughing, hard blowing, smoking, or vomiting after a dental surgery can cause subcutaneous emphysema. During procedures requiring anesthesia, tearing of the tracheal mucosa during intubation or increased pressure in the alveoli because of excessive ventilation pressure can lead to introduction of air into the pleural and mediastinal spaces. The presenting signs and symptoms of subcutaneous emphysema after a procedure vary. Other incidents took place minutes to hours after the treatment was finished, although some reports highlight almost instantaneous signs and symptoms. Patients with subcutaneous emphysema have significant swelling and discomfort when subcutaneous tissue has been pierced by air, as well as respiratory changes if the condition has extended to the paratracheal, mediastinal, or thoracic regions. Crepitus on palpation, the pathognomonic symptom of subcutaneous emphysema, enables rapid exclusion of allergic reactions or angioedema in cases of acute swelling. As soon as subcutaneous emphysema is identified, a radiographic examination of the patient should be done to ascertain the degree and location of the emphysema. Prior to release, patients with clinically substantial subcutaneous emphysema should have their respiratory and heart health continuously evaluated. Despite being concerning, most cases of subcutaneous emphysema often cure on their own within 3–5 days without any problems or morbidities, and fully recover within 7–10 days [4],[10].
To avoid subcutaneous emphysema, doctors should abide by the air-driven turbine manufacturer’s instructions for use and maintenance. Additionally, after a dental or surgical surgery, postoperative instructions should specify to refrain from coughing, smoking, blowing one’s nose, using straws, vomiting, or engaging in any other action that can create pressure in the oral cavity. Antibiotics are prescribed to protect against germs that air from an intraoral location may introduce and which may cause necrotizing fasciitis. Rarely surgical intervention is necessary after diagnosis of subcutaneous emphysema. In isolated cases the need for exploratory surgery, emergency tracheotomy, and placement of chest tubes has been reported [4].
Infection is not usually observed in these cases, and surgical treatment is not usually needed. However, it’s important to be aware of the possibility that utilizing air-powder abrasive equipment could result in iatrogenic emphysema. Given the frequent use of air-powder abrasive devices to treat peri-implantitis, there is a chance for infection. The spread of oral, pharyngeal, or tonsillar abscesses, as well as osteomyelitis of the facial bones or infections of the salivary glands, are typical causes of other infectious etiologies. Dentists might isolate the tooth using specialized tools, such as rubber dams, to avoid such issues. If a dental iatrogenic cause is determined to be most likely based on the patient’s medical history, the doctor may decide to monitor the patient in the emergency room or consider admitting them. Although they are uncommon, invasive diseases like necrotizing fasciitis or mediastinitis should be taken into account because they can be fatal if not treated quickly.
Conclusion
In conclusion, subcutaneous emphysema and pneumomediastinum are potential complications of procedures using high speed dental handpieces that interrupt the epithelium of the oral cavity and introduces air, under pressure, along or into the head and neck’s fascial spaces. Iatrogenic subcutaneous emphysema is uncommon but can have serious and even fatal consequences. To lessen the likelihood of subsequent difficulties, subcutaneous emphysema must be early identified, comprehended, and properly handled when it does occur. Since most occurrences of face or cervical edema after dental treatments are misdiagnosed and the repercussions could be fatal, physicians must be able to identify and treat these issues. The use of conservative treatment has proven to be risk-free. Given the gravity of this scenario, a strong clinical suspicion for an invasive necrotizing infection is still needed, but the clinician’s judgement should be used to decide whether to pursue close observation or surgical exploration.
REFERENCES
1.
Monsour PA, Savage NW. Cervicofacial emphysema following dental procedures. Aust Dent J 1989;34(5):403–6. [CrossRef]
[Pubmed]

2.
Horowitz I, Hirshberg A, Freedman A. Pneumomediastinum and subcutaneous emphysema following surgical extraction of mandibular third molars: Three case reports. Oral Surg Oral Med Oral Pathol 1987;63(1):25–8. [CrossRef]
[Pubmed]
3.
Arai I, Aoki T, Yamazaki H, Ota Y, Kaneko A. Pneumomediastinum and subcutaneous emphysema after dental extraction detected incidentally by regular medical checkup: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107(4):e33–8. [CrossRef]
[Pubmed]
4.
McKenzie WS, Rosenberg M. Iatrogenic subcutaneous emphysema of dental and surgical origin: A literature review. J Oral Maxillofac Surg 2009;67(6):1265–8. [CrossRef]
[Pubmed]
5.
Brzycki RM. Case report: Subcutaneous emphysema and pneumomediastinum following dental extraction. Clin Pract Cases Emerg Med 2021;5(1):58–61. [CrossRef]
[Pubmed]
6.
Maunder RJ, Pierson DJ, Hudson LD. Subcutaneous and mediastinal emphysema. Pathophysiology, diagnosis, and management. Arch Intern Med 1984;144(7):1447–53.
[Pubmed]
7.
Rawlinson RD, Negmadjanov U, Rubay D, Ohanisian L, Waxman J. Pneumomediastinum after dental filling: A rare case presentation. Cureus 2019;11(9):e5593. [CrossRef]
[Pubmed]
8.
Busuladzic A, Patry M, Fradet L, Turgeon V, Bussieres M. Cervicofacial and mediastinal emphysema following minor dental procedure: A case report and review of the literature. J Otolaryngol Head Neck Surg 2020;49(1):61. [CrossRef]
[Pubmed]
9.
Ali A, Cunliffe DR, Watt-Smith SR. Surgical emphysema and pneumomediastinum complicating dental extraction. Br Dent J 2000;188(11):589–90. [CrossRef]
[Pubmed]
10.
Reiche-Fischel O, Helfrick JF. Intraoperative life-threatening emphysema associated with endotracheal intubation and air insufflation devices: Report of two cases. J Oral Maxillofac Surg 1995;53(9):1103–7. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Arun Nadarajah - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tzu-Yi (Arron) Chuang - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tim Elston - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Arun Nadarajah et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}