 |
Case Report
The appendix: An unexpected band obstruction
1 Department of General Surgery, Westmead Hospital, Westmead, NSW 2145, Australia
Address correspondence to:
Rowan Klein Nulend
Westmead Hospital, Corner Hawkesbury Rd and Darcy Rd, Westmead, NSW 2145,
Australia
Message to Corresponding Author
Article ID: 100129Z12RN2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Klein Nulend R, Quinn R, Fok KY, Pathmanathan N. The appendix: An unexpected band obstruction. J Case Rep Images Surg 2024;10(1):6–9.ABSTRACT
Introduction: Small bowel obstruction (SBO) is common surgical pathology, most commonly secondary to adhesions. This case presents a novel cause of small bowel obstruction.
Case Report: We present a case of an elderly female who presented to hospital with symptoms, signs, and radiological findings consistent with SBO. After failing non-operative management, and deteriorating clinically, decision was made for operative intervention. A laparotomy revealed a normal-appearing appendix adhering to the pelvic side wall, and consequently forming a band adhesion-like internal hernia and was the cause of the bowel obstruction. Following dissection from the pelvic wall, and appendectomy, the patient recovered and was discharged home. Histopathology demonstrated a normal appendix. Diseased appendices have rarely been described to cause bowel obstructions; however, this is the first case report describing a normal appendix causing a band-like bowel obstruction. Surgical management was necessary to establish a definitive diagnosis, and for resolution of the condition.
Conclusion: This case highlights a novel cause of SBO and reiterates the heterogeneity of SBO causes. Abdominal exploration remains the gold standard diagnostic modality for intra-abdominal pathology.
Keywords: Appendix, Band, Internal hernia, Small bowel obstruction
Introduction
A female in her late 80s presented to the emergency department with a one-day history of right lower quadrant pain and obstructive symptoms. She had a significant past surgical history of a hysterectomy and salpingectomy in her 30s for uterine fibroids. She was co-morbid with past medical history including insulin dependent type 2 diabetes mellitus, rheumatic valvular heart disease, mitral stenosis with associated severe pulmonary hypertension and chronic kidney disease.
Case Report
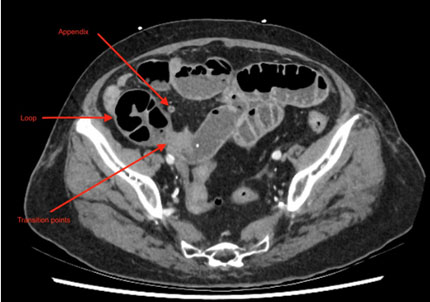
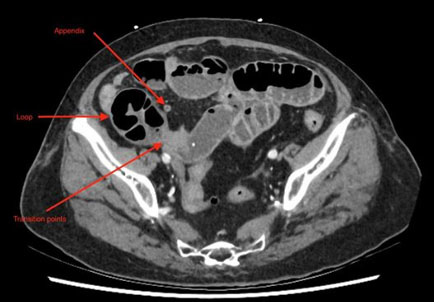
On presentation, she was hemodynamically stable, afebrile. Her abdominal examination revealed a soft, distended abdomen, with right lower quadrant tenderness and no peritonism. She had a lower midline laparotomy scar, and nil palpable hernias. A computed tomography (CT) abdomen-pelvis demonstrated a distal small bowel obstruction (SBO) with a transition point in the right lower quadrant, with trace free fluid (Figure 1, Figure 2, Figure 3, Figure 4).
She was initially managed non-operatively as an adhesional SBO; however, failed to progress. On day 4 of admission, she developed fever and her C-reactive protein (CRP) rose to 114 mg/L (from 64 mg/L), and the decision was made for operative intervention.
A laparotomy was performed. There were adhesions between the omentum and anterior abdominal wall. Following division of these adhesions, the SBO transition point was identified, which revealed the appendix tip adherent to the pelvic side wall. This normal-looking appendix was forming a band around the small bowel and creating an internal hernia, similar to a band adhesion. The appendix tip was released from the pelvic wall, and appendectomy was performed. The bowel contained within the internal hernia was viable and no resection was required.
Following her operation, she was admitted to intensive care unit (ICU) due to her extensive comorbidities putting her at a high peri-operative risk. The patient’s post-operative course was complicated by a urinary tract infection and aspiration pneumonia, each of which resolved quickly with antimicrobial therapy. There were no surgical complications. Following rehabilitation, she was discharged home on post-operative day 16.
The appendix histopathology revealed a normal appendix, without any evidence of inflammation, dysplasia, or malignancy.


Discussion
Small bowel obstruction (SBO) is a common intra-abdominal pathology and can be attributed to a large range of causes, the most common of which is intra-abdominal adhesions. Given the associated morbidity and occurrence of adhesions, there is significant emphasis on prevention of adhesions, which includes both technical measures and physical barriers. For patients undergoing gynecological surgery, as was this patient’s history, solid physical barriers are likely to be most effective [1].
Other common causes include, yet are not limited to, incarcerated hernias, malignancy, Crohn disease, foreign bodies, and volvulus [2].
The appendix is another common source of intra-abdominal pathology, or “the acute abdomen.” Generally this is as a result of appendicitis or associated complications including phlegmon, abscess or perforation. Other appendiceal pathologies, including other inflammatory processes, or non-inflammatory conditions such as neoplasia are less common [3].
There are very rare reports of SBO secondary to appendiceal pathology. This has been labeled with a range of titles including “appendiceal banding,” “appendiceal knotting,” “appendiceal tourniquet,” or “appendiceal tie.” Each of these terms describes a process where the appendix has formed an adhesion-like band, and wrapped around or adhered to the small bowel in a manner where this has caused extra-luminal obstruction, resulting in a clinical SBO.
The vast majority of these cases were in the setting of acute appendicitis [4],[5],[6],[7],[8],[9],[10],[11],[12]. Makama et al. conducted a review on acute appendicitis causing SBO; however, this review does not note any cases of a normal appendix causing SBO [13]. In these settings, it is hypothesized that the architectural changes in the context of local inflammation result in the appendix adhering to, or around the small bowel, causing mechanical SBO [13].
Less frequency cases occurred secondary to other pathology affecting the appendix. These cases included previous non-operatively managed appendicitis [14], chronic inflammation [15], anatomical variation [16], and one report involves a case of endometriosis affecting the appendix and subsequently forming a band around terminal ileum [17].
All of these cases were managed operatively, either with laparoscopy (five cases) or laparotomy (eight cases). Exact procedures performed differed depending on the exact underlying cause, the extent of the subsequent bowel obstruction and associated bowel viability; however, each procedure included an appendectomy. Four patients required bowel resection.
To our knowledge, no reports describe a SBO secondary to an appendiceal band in the absence of appendiceal pathology. Our patient’s appendix appeared normal both macroscopically and microscopically.
In this patient’s case, she may have been pre-disposed to this condition by her previous hysterectomy and associated pelvic adhesions. Unlike other cases, however, she had no pathology affecting the appendix directly, nor did she have a history of non-operatively managed appendicitis.
Computed tomography abdomen was a helpful tool to diagnose the patient’s SBO, however, did not reveal the appendix as the underlying cause. Definitive diagnosis and management required abdominal exploration.
Conclusion
Overall, this case highlights a novel cause of SBO, and reiterates the heterogeneity of SBO causes, and that there should always be a high degree of suspicion with presumed adhesive SBO. Abdominal exploration remains the gold standard diagnostic modality for intra-abdominal pathology.
REFERENCES
1.
Ten Broek RPG, Stommel MWJ, Strik C, van Laarhoven CJHM, Keus F, van Goor H. Benefits and harms of adhesion barriers for abdominal surgery: A systematic review and meta-analysis. Lancet 2014;383(9911):48–59. [CrossRef]
[Pubmed]

2.
Schick MA, Kashyap S, Meseeha M. Small Bowel Obstruction. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
[Pubmed]
3.
Yoo HY, Choi J, Kim J, et al. Unexpected appendiceal pathologies and their changes with the expanding use of preoperative imaging studies. Ann Coloproctol 2017;33(3):99–105. [CrossRef]
[Pubmed]
4.
Yee FZY, Cheng LTE, Wong TH. Appendiceal-tie syndrome: Acute appendicitis causing mechanical small bowel obstruction managed laparoscopically. ANZ J Surg 2019;89(11):1513–5. [CrossRef]
[Pubmed]
5.
Karlsen EA, Mulholland P, Mouline O, Cross T. Appendicular ring: An unusual cause of mechanical small bowel obstruction. ANZ J Surg 2021;91(11):E727–8. [CrossRef]
[Pubmed]
6.
Ali SM, Khalil IA, Musthafa S, Shah AA, Aftab Z, Al-Mudares S. Strangulated internal hernia through appendicular tourniquet/ring: Unusual cause of intestinal obstruction. Am J Case Rep 2020;21:e920384. [CrossRef]
[Pubmed]
7.
Menon T, Martin RJ, Cameron D, Rao S. Appendiceal tie syndrome. Australas Radiol 2007;51 Spec No.:B133–6. [CrossRef]
[Pubmed]
8.
Al-Qallaf A, Shuaib A, Al-Sharaf K, Behbehani A. Acute appendicitis as a rare cause of mechanical small bowel obstruction case report. Qatar Med J 2017;2017(2):4. [CrossRef]
[Pubmed]
9.
Awale L, Joshi BR, Rajbanshi S, Adhikary S. Appendiceal tie syndrome: A very rare complication of a common disease. World J Gastrointest Surg 2015;7(4):67–70.
[Pubmed]
10.
Bhandari L, Mohandas P. Appendicitis as a cause of intestinal strangulation: A case report and review. World J Emerg Surg 2009;4:34. [CrossRef]
[Pubmed]
11.
Chatterjee C, Dash S, Gupta S, Ghosh S. Appendiceal knotting causing small bowel strangulation. J Res Med Sci 2014;19(10):1016–7.
[Pubmed]
12.
Yang AD, Lee CH. Appendico-ileal knotting resulting in closed-loop obstruction in a child. Pediatr Radiol 2002;32(12):879–81. [CrossRef]
[Pubmed]
13.
Makama JG, Kache SA, Ajah LJ, Ameh EA. Intestinal obstruction caused by appendicitis: A systematic review. J West Afr Coll Surg 2017;7(3):94–115.
[Pubmed]
14.
Donovan A, Tabone R, Yuide PJ, Chua TC. Small bowel obstruction from an appendiceal tie. ANZ J Surg 2020;90(9):1796–8. [CrossRef]
[Pubmed]
15.
O’Donnell ME, Sharif MA, O’Kane A, Spence RAJ. Small bowel obstruction secondary to an appendiceal tourniquet. Ir J Med Sci 2009;178(1):101–5. [CrossRef]
[Pubmed]
16.
Bali R, Wani M, Mir S, Thakur S, Bhat R. Appendiceal duplication with simultaneous acute appendicitis and appendicular perforation causing small bowel obstruction. J Surg Case Rep 2011;2011(2):3. [CrossRef]
[Pubmed]
17.
Choi JDW, Yunaev M. Endometriosis of the appendix causing small bowel obstruction in a virgin abdomen. BMJ Case Rep 2019;12(7):e230496. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Rowan Klein Nulend - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rakesh Quinn - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kar Yin Fok - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nimalan Pathmanathan - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Rowan Klein Nulend et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}