 |
Case Report
Massive renal pelvis urothelial carcinoma with invasion of the descending colon and cutaneous metastases: A case report and literature review
1 Department of Urology, Taitung Mackay Memorial Hospital, Taitung, Taiwan
2 Department of Medicine, Mackay Medical College, New Taipei City, Taiwan
3 Department of Colorectal Surgery, Taitung Mackay Memorial Hospital, Taitung, Taiwan
4 Department of General Surgery, Taitung Mackay Memorial Hospital, Taitung, Taiwan
5 Department of Pathology, Taitung Mackay Memorial Hospital, Taitung, Taiwan
Address correspondence to:
Ti-Yuan Yang
No. 1, Ln. 303, Changsha St., Taitung City, Taitung County,
Taiwan
Message to Corresponding Author
Article ID: 100135Z12TY2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Yang TY, Hung YT, Huang SS, Chu CY. Massive renal pelvis urothelial carcinoma with invasion of the descending colon and cutaneous metastases: A case report and literature review. J Case Rep Images Surg 2024;10(1):34–38.ABSTRACT
Introduction: Skin metastases and gastrointestinal tract involvement in upper tract urothelial carcinoma (UTUC) are uncommon and associated with an adverse prognosis. This report details a case of extensive urothelial carcinoma originating from the renal pelvis, invading the descending colon, and presenting with cutaneous metastases.
Case Report: A 63-year-old male patient visited the emergency department on the account of sudden onset of severe left upper abdominal pain and nausea. The computed tomography (CT) revealed soft tissue density at the mesentery adjacent to the left kidney with the involvement of the distal transverse colon. The patient underwent left radical nephroureterectomy, left hemicolectomy, and bladder cuff excision. Six weeks postoperatively, left inguinal cutaneous metastases, approximately 4 cm, were excised. Due to renal dysfunction, the patient received gemcitabine and carboplatin chemotherapy, followed by pembrolizumab for the cutaneous metastatic disease. Follow-up imaging showed no evidence of recurrence or metastasis 15 months postoperatively.
Conclusion: In cases of advanced UTUC, a multidisciplinary approach combining surgical intervention, chemotherapy, and immunotherapy can alleviate symptoms and potentially improve survival rates. This integrative treatment strategy highlights the importance of a multidisciplinary approach in managing complex oncological cases.
Keywords: Cutaneous metastases, Nephroureterectomy, Upper tract urothelial carcinoma
Introduction
Upper tract urothelial carcinoma (UTUC) accounts for 5–10% of all cases of urothelial cancers in Western countries. However, Taiwan has been considered an endemic region wherein UTUC accounts for 23–30% of all cases of urothelial tumors [1],[2],[3]. Upper tract urothelial carcinoma extending to the gastrointestinal tract or cutaneous metastases is rare. A literature review has found that numerous cases presented with either UTUC skin metastases or gastrointestinal tract invasion. However, concomitant cutaneous metastases and gastrointestinal tract involvement were not observed [4],[5],[6],[7],[8],[9]. In this study, we report a massive urothelial carcinoma in the renal pelvis that had extended to the descending colon and had been associated with cutaneous metastases. The patient underwent radical nephroureterectomy, left hemicolectomy, bladder cuff excision, and skin tumor excision.
Case Report
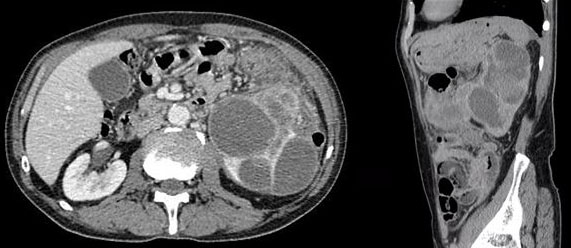
In November 2022, a 63-year-old male patient visited the emergency department on the account of sudden onset of severe left upper abdominal pain and nausea. During physical examination, tenderness and a hard, palpable mass were found in the left upper abdominal region. The contrast-enhanced CT of the abdomen and pelvis revealed soft tissue density at the mesentery adjacent to the left kidney with the involvement of the distal transverse colon (Figure 1A and Figure 1B).
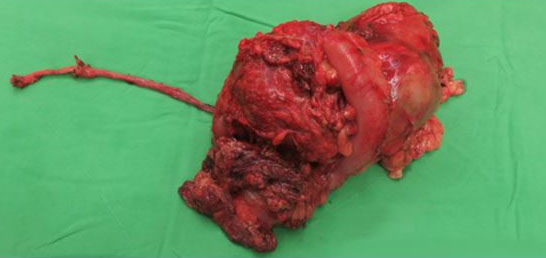
Under general endotracheal anesthesia, the patient was placed in the lithotomy position. The transurethral resection of the intramural ureter deep into the extravesical fat was performed using a Collins knife. The patient was then placed in the supine position, open surgical approach was undertaken with upper midline laparotomy. The left colic vessels and left branch of the middle colic vessels were ligated, and a side-to-side anastomosis was created using a 60-mm Endo-GIA stapler. The left renal vein and renal artery were clamped and divided using a 45-mm Endo-GIA stapler. The ureter was placed under gentle traction to pull it away from the bladder. Para-aortic lymphadenectomy was precluded by severe adhesions and the associated risks of bleeding and aortic injury. The surgical specimen consisted of the kidney, ureter, bladder cuff, and attached colon (Figure 2).
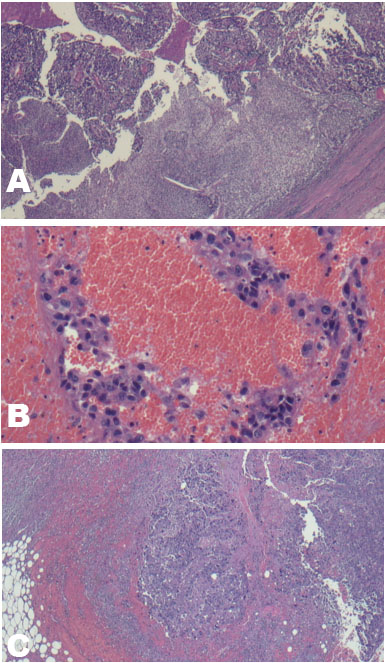
The histopathological analysis of the specimens suggested the presence of high-grade urothelial carcinoma. The tumor had a size of up to 14.2 cm in the most significant dimension and involved the proximal part of the ureter, renal pelvis, and renal parenchyma and extended to the kidney into the mesentery of the colon (Figure 3A and Figure 3B). A lymph node with metastatic carcinoma was found within the hilum. The surgical margin was microscopically negative.
He was discharged 11 days after the operation. Due to renal dysfunction (eGFR 24–50 mL/min), he was ineligible for standard cisplatin-based chemotherapy. Chemotherapy was started in December 2022, consisting of gemcitabine (1000 mg/m2, D2/9), and carboplatin (area under the curve of 6, D3), every three weeks. Six weeks post-operatively, the patient complained of a growing, nontender, hard nodule approximately 4 cm in size over the left inguinal area. He had noticed mild skin swelling for a few months but initially thought it was just acne and did not pay much attention to it. In the preoperative CT scans, no suspected cutaneous metastasis was detected. The excision of the skin and soft tissue was performed, and the histopathological examination results revealed the presence of metastatic carcinoma of urothelial origin (Figure 3C). The surgical section margin is free and programmed cell death-ligand 1 (PD-PDL1) positive. The CT and bone scans that were performed three and nine months after the left nephroureterectomy and left hemicolectomy showed no evidence of recurrence or metastasis. The patient was alive 15 months postop and was administered with 200 mg pembrolizumab every three weeks for cutaneous metastatic urothelial cell carcinoma.
Discussion
Upper tract urothelial carcinoma is a relatively rare disease, and five-year disease-specific survival rates fall below 50% for stages pT2/pT3 and are less than 10% for stage pT4 UTUC [10]. Miyazato et al. reported a 47-year-old man with left renal pelvis urothelial carcinoma and inferior vena cava thrombus [4]. Moreover, they also conducted a literature review and found 17 other cases with tumor thrombus in the vena cava. However, none of the patients presented with gastrointestinal tract invasion. Li et al. reported 3 cases and reviewed 34 cases of venous tumor thrombus that were discussed in 26 studies [5]. None of the tumors had directly invaded the gastrointestinal tract, even in these advanced cancer patients.
Nikfarjam et al. reported an 83-year-old female patient with a 4-cm right renal urothelial carcinoma attached to the duodenum [6]. The patient underwent right nephrectomy, pylorus-preserving pancreaticoduodenectomy, and adrenalectomy and was alive and disease free after three months. Nakano et al. reported the first case of a sarcomatoid type of renal pelvis urothelial carcinoma with the direct invasion of the pancreas and descending colon [7]. A 75-year-old woman presented with leukocytosis and lost approximately 4 kg in two months. The contrast-enhanced CT revealed a 6.1-cm left upper pole renal tumor and suspected left renal cell carcinoma with pancreatic and splenic infiltration. Moreover, left nephrectomy was performed, and the pancreatic tail, spleen, and 20-cm descending colon were removed. The histopathological examination results revealed an invasive urothelial carcinoma with sarcomatoid differentiation. Postoperative chemotherapy with gemcitabine and carboplatin was performed. However, the patient expired at five months after surgery.
Cutaneous metastases from genitourinary tract cancer are rare and occur in 1.3% of cases with primary urologic malignancies [8]. Singh et al. reported a 70-year-old woman with metastatic urothelial carcinoma from the renal pelvis to the abdominal skin and reviewed six cases published in the literature [9]. Four of the seven patients died within three months.
Compared with open radical nephroureterectomy, laparoscopic radical nephroureterectomy offers the advantages of minimally invasive surgery without deteriorating the oncological outcomes [11],[12]. However, based on the current available evidence, laparoscopic radical nephroureterectomy may yield inferior oncological outcomes compared with open radical nephroureterectomy when the bladder cuff is excised laparoscopically, especially in patients with locally advanced high-risk UTUC (pT3/pT4 and/or high-grade) [13]. Considering the anatomical limitations, the colon cannot be resected through the retroperitoneal space. In patients with metastatic UTUC, the combination of nephroureterectomy and chemotherapy has resulted in superior survival outcomes compared with chemotherapy alone [14]. Therefore, in this study, it is a reasonable option to use a transperitoneal open procedure when colon invasion is suspected. Furthermore, it was concluded that surgical intervention not only improves the abdominal pain symptoms but also offers potential survival benefits.
Lymph node dissection during radical nephroureterectomy for upper tract urothelial carcinoma allows for optimal tumor staging, although its survival benefit remains controversial [15],[16],[17]. In cN+ UTUC patients, focusing on pNx and pN+, lymph node dissection offers no overall survival benefit; however, adjuvant chemotherapy is correlated with improved survival outcomes in cN+ patients [17]. Use of a lymph node dissection template is likely to have a greater impact on cancer-specific survival than the number of lymph nodes removed, and the degree of completeness improves cancer-specific survival and reduces the risk of local recurrence [18],[19]. For left renal pelvis UTUC, complete lymphadenectomy should encompass both the renal hilar and para-aortic nodes [20]. In the case presented, CT imaging disclosed no evidence of para-aortic lymphadenopathy. Owing to significant adhesion surrounding the aorta, potentially related to hydronephrosis and secondary pyelonephritis, attempts to perform a comprehensive para-aortic lymph node dissection were met with persistent bleeding and concerns regarding potential damage to the aorta, which compelled us to terminate the procedure. In scenarios where feasible, a template-based lymphadenectomy should be executed wherever possible in patients with presumed muscle-invasive UTUC [10],[19].
Conclusion
Based on the literature, many cases have been presented with either UTUC skin metastases or gastrointestinal tract invasion. However, no cases with concurrent cutaneous metastases and gastrointestinal tract involvement have been identified. To our knowledge, our patient is the first case of renal pelvis urothelial carcinoma extending to the descending colon and cutaneous metastases. Considering the poor prognosis of the patient in relation to skin metastases or gastrointestinal tract invasion, follow-up monitoring is necessary.
REFERENCES
1.
Soria F, Shariat SF, Lerner SP, et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J Urol 2017;35(3):379–87. [CrossRef]
[Pubmed]

2.
Chen IA, Chang CH, Huang CP, et al. Factors predicting oncological outcomes of radical nephroureterectomy for upper tract urothelial carcinoma in Taiwan. Front Oncol 2022;11:766576. [CrossRef]
[Pubmed]
3.
Tan LB, Chang LL, Cheng KI, Huang CH, Kwan AL. Transitional cell carcinomas of the renal pelvis and the ureter: Comparative demographic characteristics, pathological grade and stage and 5-year survival in a Taiwanese population. BJU Int 2009;103(3):312–6. [CrossRef]
[Pubmed]
4.
Miyazato M, Yonou H, Sugaya K, Koyama Y, Hatano T, Ogawa Y. Transitional cell carcinoma of the renal pelvis forming tumor thrombus in the vena cava. Int J Urol 2001;8(10):575–7. [CrossRef]
[Pubmed]
5.
Li M, Shi A, Kong W, et al. Transitional cell carcinoma with extension of the renal vein and IVC tumor thrombus: Report of three cases and literature review. World J Surg Oncol 2016;14(1):309. [CrossRef]
[Pubmed]
6.
Nikfarjam M, Gusani NJ, Kimchi ET, Mahraj RP, Staveley-O’Carroll KF. Combined right nephrectomy and pancreaticoduodenectomy. Indications and outcomes. JOP 2008;9(4):449–55.
[Pubmed]
7.
Nakano Y, Kitano H, Hieda K, et al. Sarcomatoid variant of urothelial carcinoma of renal pelvis with direct invasion of the pancreas and descending colon. IJU Case Rep 2022;5(5):350–3. [CrossRef]
[Pubmed]
8.
Mueller TJ, Wu H, Greenberg RE, et al. Cutaneous metastases from genitourinary malignancies. Urology 2004;63(6):1021–6. [CrossRef]
[Pubmed]
9.
Singh P, Kolte S, Singh GK. Cytological diagnosis of a rare case of cutaneous metastasis from transitional cell carcinoma, renal pelvis. J Egypt Natl Canc Inst 2017;29(4):197–200. [CrossRef]
[Pubmed]
10.
Rouprêt M, Babjuk M, Burger M, et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur Urol 2021;79(1):62–79. [CrossRef]
[Pubmed]
11.
Favaretto RL, Shariat SF, Chade DC, et al. Comparison between laparoscopic and open radical nephroureterectomy in a contemporary group of patients: Are recurrence and disease-specific survival associated with surgical technique? Eur Urol 2010;58(5):645–51. [CrossRef]
[Pubmed]
12.
Walton TJ, Novara G, Matsumoto K, et al. Oncological outcomes after laparoscopic and open radical nephroureterectomy: Results from an international cohort. BJU Int 2011;108(3):406–12. [CrossRef]
[Pubmed]
13.
Peyronnet B, Seisen T, Dominguez-Escrig JL, et al. Oncological outcomes of laparoscopic nephroureterectomy versus open radical nephroureterectomy for upper tract urothelial carcinoma: An European Association of Urology Guidelines Systematic Review. Eur Urol Focus 2019;5(2):205–23 [CrossRef]
[Pubmed]
14.
Lin WY, Lin MH, Yang YH, et al. Survival impact of nephroureterectomy for de novo Stage IV nonmetastatic and metastatic upper tract urothelial carcinoma. Front Surg 2022;9:903123. [CrossRef]
[Pubmed]
15.
Roscigno M, Brausi M, Heidenreich A, et al. Lymphadenectomy at the time of nephroureterectomy for upper tract urothelial cancer. Eur Urol 2011;60(4):776–83. [CrossRef]
[Pubmed]
16.
Nazzani S, Mazzone E, Preisser F, et al. Rates of lymph node invasion and their impact on cancer specific mortality in upper urinary tract urothelial carcinoma. Eur J Surg Oncol 2019;45(7):1238–45. [CrossRef]
[Pubmed]
17.
Piontkowski AJ, Corsi N, Morisetty S, et al. Benefit of lymph node dissection in cN+ patients in the treatment of upper tract urothelial carcinoma: Analysis of NCDB registry. Urol Oncol 2022;40(9):409.e9–17. [CrossRef]
[Pubmed]
18.
Dong F, Xu T, Wang X, et al. Lymph node dissection could bring survival benefits to patients diagnosed with clinically node-negative upper urinary tract urothelial cancer: A population-based, propensity score-matched study. Int J Clin Oncol 2019;24(3):296–305. [CrossRef]
[Pubmed]
19.
Rouprêt M, Seisen T, Birtle AJ, et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. Eur Urol 2023;84(1):49–64. [CrossRef]
[Pubmed]
20.
Kondo T, Hashimoto Y, Kobayashi H, et al. Template-based lymphadenectomy in urothelial carcinoma of the upper urinary tract: Impact on patient survival. Int J Urol 2010;17(10):848–54. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ti-Yuan Yang - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yu-Ting Hung - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shou-Sen Huang - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Chia-Ying Chu - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Ti-Yuan Yang et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}