 |
Case Report
Concurrent presentation of unrelated perforated appendicitis and high-grade small bowel obstruction: A case report
1 Department of Surgery, Swedish Medical Center, 501 E. Hampden Ave, Englewood, CO 80113, USA
Address correspondence to:
Samantha Greenseid
Department of Surgery, Swedish Medical Center, 501 E. Hampden Ave, Englewood, CO 80113,
USA
Message to Corresponding Author
Article ID: 100141Z12SG2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Greenseid S, Moody A, Quan G. Concurrent presentation of unrelated perforated appendicitis and high-grade small bowel obstruction: A case report. J Case Rep Images Surg 2024;10(2):10–13.ABSTRACT
Small bowel obstruction and acute perforated appendicitis are common surgical problems independently. At times, acute appendicitis may present with small bowel obstruction due to the localized inflammatory process. This results in mechanical small bowel obstruction usually near the terminal ileum. However, it is extremely rare to have both abdominal processes occurring simultaneously, but not related to one another. In this study, we present a case of a healthy 62-year-old female patient who had concurrent high-grade small bowel obstruction due to a chronic adhesive band and perforated appendicitis, seemingly completely independent of each other.
Keywords: Perforated appendicitis, Periumbilical pain, Small bowel obstruction
Introduction
Acute appendicitis and small bowel obstruction are both very common pathologies that are seen by general surgeons. The lifetime risk of appendicitis is 8.6% in males and 6.7% in females [1],[2]. Symptoms include periumbilical pain that radiates and localizes to the right lower quadrant of the abdomen, abdominal distension or rigidity, and fever. Small bowel obstructions are often seen in the emergency department (ED) and warrant a general surgery consultation. Symptoms include severe abdominal pain that may be generalized or localized to the area of obstruction. Patients often had not had a bowel movement or passed flatus for some length of time, and may experience severe nausea and vomiting. Obstructions can be caused by both mechanical and non-mechanical mechanisms. The most common mechanism of obstruction is adhesions [3].
Although both pathologies are commonly seen individually, it is unlikely for a patient to present with unrelated pathologies simultaneously. Perforated appendicitis can cause ileus or even obstruction in the bowel located in the same area as the perforation due to inflammation and adhesions. This patient had an adhesion distant from the site of perforation and completely unrelated.
Case Report
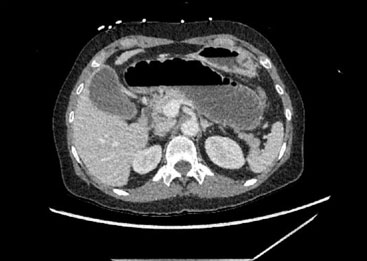
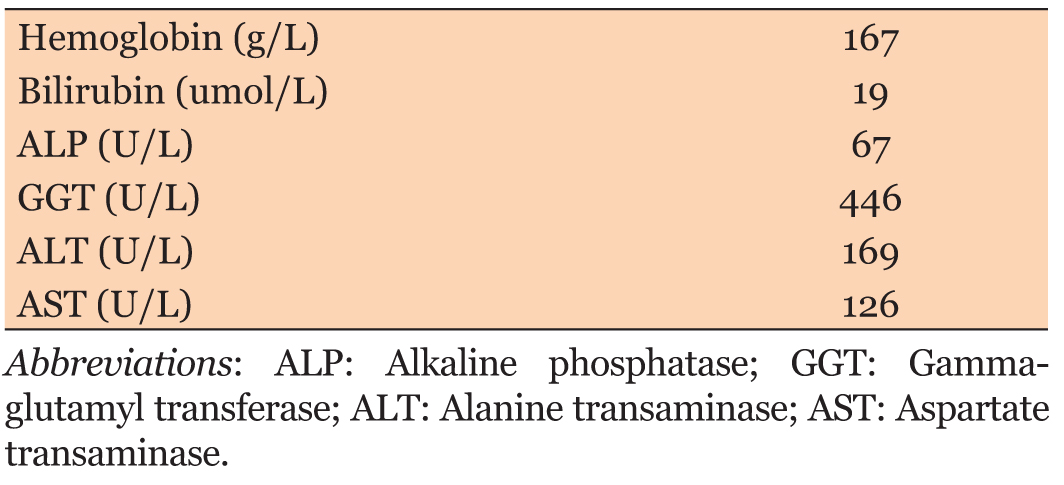
A 62-year-old otherwise healthy female patient with a surgical history significant for open hysterectomy many years prior presented to the emergency room with six days of abdominal pain and associated nausea and vomiting. She endorsed a subjective fever three days prior to presentation and her last bowel movement was the day prior to presentation, which was described as normal. Of note, the patient’s last colonoscopy was three years ago and reported as normal. On physical examination, her abdomen was soft and only mildly tender to palpation of the middle abdomen, no distention, no guarding, and no peritonitis was present on initial examination. Her vital signs were normal, without fever, tachycardia, or hypotension. Initially, her lactic acid was elevated to 4.2 but improved to 2.1 with intravenous fluid administration. She did have a leukocytosis of 11.6 and her creatinine was elevated to 1.7. On computed tomography (CT) of her abdomen and pelvis, there was a high grade small bowel obstruction located in the mid-jejunum (Figure 1) and two separate pelvic fluid collections with rim-enhancement concerning for abscesses (Figure 2). Upon further review of the imaging with the on-call radiologist, he recognized that the appendix appeared to have lack of mucosal enhancement with surrounding inflammatory stranding. With the adjacent pelvic fluid collections, there was concern for perforated appendicitis as well. We then had a discussion with her and her family member that we were concerned two separate processes were occurring in her abdomen. Despite the patient’s non-toxic clinical exam, the decision was made to urgently take the patient to the operating room to explore her abdomen. Intraoperatively, we discovered perforated appendicitis (Figure 3) with purulent fluid collections in the pelvis. At this point, we performed an open appendectomy. We then turned our attention to the small bowel obstruction. The small bowel was eviscerated and with gentle manipulation, a chronic-appearing adhesive band located between a loop of mid-jejunum was lysed with finger dissection. This appeared to be a closed-loop small bowel obstruction. The small bowel was dilated and mildly hemorrhagic, but appeared viable, so no bowel resection was performed.
There was no surrounding inflammation involving the small bowel to suggest that the adhesive band was a result of the perforated appendicitis. Postoperatively, she had a nasogastric tube (NGT) for decompression given the dilated small bowel and infectious process, likely leading to an ileus. She had return of bowel function on postoperative day 4. Her NGT was removed and her diet was advanced as tolerated. The patient recovered well and was discharged home postoperative day 6. Skin staples were removed postoperative day 14 at her clinic follow up visit.


Discussion
Mechanical small bowel obstruction caused by acute appendicitis is rare. This usually results from the acute inflammatory response in close approximation to the appendix, causing a nearby mechanical obstruction [1]. The first reported cases of mechanical small bowel obstruction caused by acute appendicitis was in 1901 by Lucius Hotchkiss in a report in which he presented three operative cases [4]. There are a few case reports describing concomitant acute appendicitis, perforated and non-perforated, and mechanical small bowel obstruction, but to our knowledge there has been no documented cases of completely unrelated perforated acute appendicitis and small bowel obstruction, not being the result of one another. This presentation of acute appendicitis and small bowel obstruction may easily be overlooked as two separate diagnoses. Failure to connect the two in such a case as this can oftentimes result in delays in diagnosis and treatment.
It is common to have varying degrees of bowel distention, usually caused by small bowel ileus, with acute appendicitis [1]. In their literature review of 10 case reports, Harrison et al. mention that differentiating between ileus and mechanical small bowel obstruction due to acute appendicitis is difficult to do clinically. In almost all of the case reports that were reviewed in this study, the source of the small bowel obstruction was an adhesive band adjacent to the terminal ileum and caused by acute and chronic inflammation of the appendix.
In 2009, Bhandari described four different mechanisms in which mechanical small bowel obstruction due to appendicitis results; adynamic, mechanical, strangulation, and ischemia [5]. Adynamic, or paralytic ileus, is the most common at 1–5% due to periappendicular inflammation causing temporary ileus. True ileus very rarely requires operative intervention alone [6]. Mechanical obstruction without strangulation is most often caused by kinking, compression or traction of the small bowel due to periappendiceal abscess acutely or adhesions that occur months to years after the initial presentation of appendicitis. Strangulation of the small bowel is rare, but may be caused by the appendix wrapping around nearby omentum, colon, or posterior peritoneum due to, again, the acute inflammatory response. This leads to small bowel herniating through the defect. Ischemia causing small bowel obstruction is extremely rare with only one case reported in 1969 by Gupta [7]. This case demonstrated an inflamed appendix that was adhered to the mesentery, causing ileocolic artery thrombosis and necrosis of the terminal ileum.
In our case presentation, the patient had several risk factors for developing mechanical small bowel obstruction due to acute appendicitis, such as abscess and localized inflammatory response. However, our patient clearly had a distinct transition point far away from the inflammatory process in her pelvis and right lower quadrant, as evidenced by a single adhesion in her proximal jejunum with no fibrinous slough or inflammatory response in this area. We describe the case above to caution providers not to overlook a diagnosis of acute appendicitis, and small bowel dilation with symptoms concerning for small bowel obstruction as simply a process likely due to adynamic ileus. If clinical suspicion is high for both acute appendicitis and mechanical small bowel obstruction, operative intervention is warranted.
Conclusion
This case highlights a rare and instructive instance of simultaneous acute perforated appendicitis and high-grade small bowel obstruction occurring independently of one another. The presented patient had a chronic adhesive band causing mechanical obstruction in the mid-jejunum, unrelated to the inflammation and perforation of the appendix. This case underscores the importance of considering multiple, potentially unrelated abdominal pathologies in patients presenting with symptoms that could be attributed to either condition individually.
In clinical practice, while mechanical obstruction due to appendicitis is a recognized phenomenon, it is exceedingly uncommon for these conditions to occur entirely independently, as demonstrated here. The presence of a distinct transition point away from the site of appendiceal inflammation emphasizes the need for thorough diagnostic evaluation when faced with complex abdominal presentations. Surgeons and clinicians should maintain a high index of suspicion and consider both acute appendicitis and other causes of bowel obstruction in differential diagnoses. Prompt operative intervention can be crucial in addressing and managing such concurrent conditions effectively, ensuring optimal patient outcomes.
REFERENCES
1.
Harrison S, Mahawar K, Brown D, Boobis L, Small P. Acute appendicitis presenting as small bowel obstruction: Two case reports. Cases J 2009;2:9106. [CrossRef]
[Pubmed]

2.
Snyder MJ, Guthrie M, Cagle S. Acute appendicitis: Efficient diagnosis and management. Am Fam Physician 2018;98(1):25–33.
[Pubmed]
3.
Long B, Robertson J, Koyfman A. Emergency medicine evaluation and management of small bowel obstruction: Evidence-based recommendations. J Emerg Med 2019;56(2):166–76. [CrossRef]
[Pubmed]
4.
Malý O, Páral J. Appendicitis as a rare cause of mechanical small-bowel obstruction: A literature review of case reports. Int J Surg Case Rep 2016;29:180–4. [CrossRef]
[Pubmed]
5.
Bhandari L, Mohandas P. Appendicitis as a cause of intestinal strangulation: A case report and review. World J Emerg Surg 2009;4:34. [CrossRef]
[Pubmed]
6.
Makama JG, Kache SA, Ajah LJ, Ameh EA. Intestinal obstruction caused by appendicitis: A systematic review. J West Afr Coll Surg 2017;7(3):94–115.
[Pubmed]
7.
Gupta S, Vaidya MP. Mechanical small bowel obstruction cause by acute appendicitis. Am Surg 1969;35(9):670–4.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Samantha Greenseid - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alexandra Moody - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Glenda Quan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Samantha Greenseid et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}