 |
Clinical Image
Bleeding jejunal ulcer and small bowel obstruction induced by a duck bone
1 Medical Officer, Ministry of Health Holdings, Singapore, Singapore; Department of General Surgery, Acute Care Surgery, Singapore General Hospital, Singapore
2 Registrar, Ministry of Health Holdings, Singapore, Singapore; Department of General Surgery, Acute Care Surgery, Singapore General Hospital, Singapore
3 Senior Consultant, Head of Department, Department of General Surgery, Acute Care Surgery, Singapore General Hospital, Singapore; Surgery Academic Clinical Program, Duke-NUS Medical School Singapore, Singapore
4 Consultant, Department of General Surgery, Acute Care Surgery, Singapore General Hospital, Singapore; Surgery Academic Clinical Program, Duke-NUS Medical School Singapore, Singapore
Address correspondence to:
Lim Teik Wen
20 College Road, Level 5 Academia, Singapore 169856,
Singapore
Message to Corresponding Author
Article ID: 100143Z12LW2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Lim TW, Yee ZYF, Mathur S, Poh RMB. Bleeding jejunal ulcer and small bowel obstruction induced by a duck bone. J Case Rep Images Surg 2024;10(2):18–21.ABSTRACT
No Abstract
Keywords: Duck bone, Patency capsule, Rectal bleeding
Case Report
An 82-year-old male presented with per-rectal bleeding. He had a significant medical history for chronic hepatitis B, chronic kidney disease, pancolonic diverticular disease, prostate cancer status post radiotherapy, intestinal obstruction secondary to a phytobezoar status post exploratory laparotomy, and removal of phytobezoar complicated by incisional hernia status post mesh repair.
He denied abdominal pain and his abdominal examination was unremarkable. Digital rectal examination and proctoscopy revealed altered blood. Hemoglobin on admission was 10.0 g/dL (normal values: 14.0–18.0 g/dL).
The patient underwent endoscopic evaluation of his rectal bleeding, for which esophagogastroduodenoscopy was unremarkable, and colonoscopy identified pancolonic diverticulosis with a descending colon polyp that was removed, but otherwise the patient had no significant source of bleeding. The impression was that of resolved diverticular bleeding. However, he had persistent per-rectal bleeding over the next week, with a repeat colonoscopy negative for colonic bleeding. The decision was then made for small bowel evaluation. In view of his history of intestinal obstruction, gastroenterology arranged for trial of a patency capsule prior to capsule endoscopy. The patient did not pass out the patency capsule, and abdominal radiographs confirmed retention of the patency capsule, precluding use of the capsule endoscopy, and gastroenterology proceed with endoscopic small bowel evaluation. Double balloon enteroscopy identified a jejunal ulcer, and hemostasis was achieved via endoscopic clipping. A nuclear medicine tagged red blood scan was also performed during this time, which confirmed no further localized sources of bleeding.
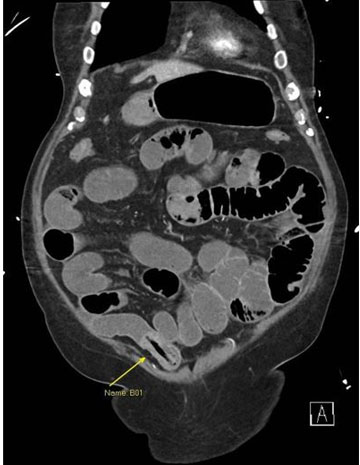
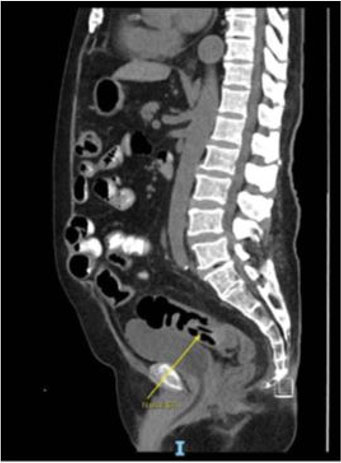
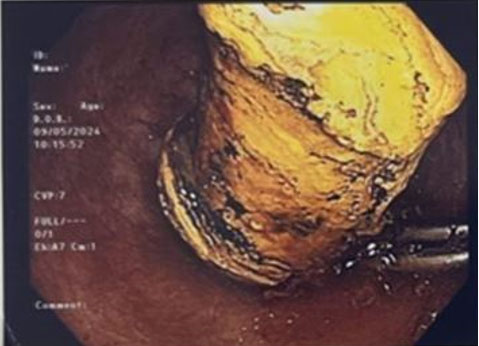
Unfortunately, the patient suffered from subsequent per-rectal bleeding with hemodynamic instability, and a computed tomographic mesenteric angiogram (CT MA) was performed which demonstrated intestinal obstruction potentially from the retained patency capsule (Figure 1). The intestinal obstruction was managed conservatively with complete resolution, and repeat CT showed migration of the foreign object to the proximal rectum (Figure 2), which required endoscopic retrieval (Figure 3). This bleeding episode resolved spontaneously with no intervention required.
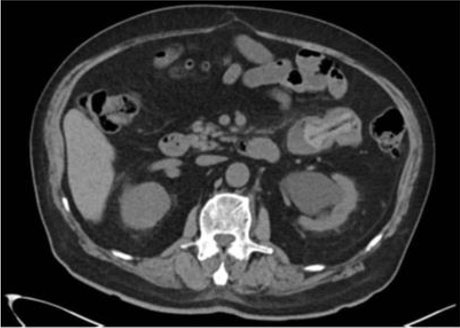
Examination of the foreign object and corroborative history from the family revealed that the foreign object was in fact a blunt duck leg bone ingested by the patient prior to admission (Figure 4). Review of a CT scan of the kidney ureters and bladder (KUB), done for acute kidney injury, prior to the ingestion of the patency capsule confirmed presence of the duck bone intra-luminally in the small intestine (Figure 5). Impression was that of a jejunal ulcer secondary to a duck bone ingestion and impaction, complicated by small bowel obstruction, confounded by the possibility of retained patency capsule. The patient was discharged home with resolution of his bleeding and intestinal obstruction.

Discussion
Gastrointestinal ulcers, obstruction, and perforation secondary to ingested foreign bodies, while uncommon, can have devastating consequences. Furthermore, in a case such as ours with persistent symptoms, attention must be paid to consider all other possibilities and not be eased into the simple likelihood of the common diverticular bleeding. Majority of perforations occur from a sharp-pointed foreign body, most commonly a fish bone, however, has also been reported to occur with the blunt natured duck bones, with one case causing bowel perforation and another anal impaction [1]. To our knowledge, there has been no case of duck bone causing gastrointestinal hemorrhage. Mechanical compression is the primary mechanism of mucosal injury in the development of bezoar-related ulcers and occurs with hard material such as this duck bone [2]. This unique case highlights a rare occurrence of ulcer development with both ensuing hemorrhage and gastrointestinal obstruction from a single duck bone.
This patient’s diagnosis was confounded by the possibility of a retained patency capsule, whereby retention and gastrointestinal obstruction is a known complication and has been reported in the literature [3]. However, the manufacturer has stated that the latest version of the patency capsule is fully dissolvable. That being said, retention of a patency capsule or capsule endoscopy needs to be on the differential list when the diagnosis remains unclear.
Furthermore, the diagnosis was delayed as knowledge of the duck bone was not offered by the patient, potentially attributable to his age and poor memory. Foreign bodies are known to be more prevalent in the elderly due to impaired swallowing controls, reduced intraoral sensitivity, as well as poorer vision and tooth loss resulting in mis-swallowing [4]. In atypical presentations such as in this case, a thorough history taking should have been considered by including the patient’s family or caregivers, as an elderly patient may not always be able to provide the clues to the underlying cause.
Conclusion
Foreign body ingestions especially in the elderly can have devastating consequences and need to be included in a clinician’s differential diagnosis in atypical presentations. A high level of clinical suspicion and thorough history taking are paramount to obtaining an accurate diagnosis. Clinicals must stay vigilant especially in cases with persistent symptoms and require a thorough diagnostic approach to consider atypical causes in such complex cases.
REFERENCES
1.
Emir S, Özkan Z, Altınsoy HB, Yazar FM, Sözen S, Bali İ. Ingested bone fragment in the bowel: Two cases and a review of the literature. World J Clin Cases 2013;1(7):212–6. [CrossRef]
[Pubmed]

2.
Oka A, Ishihara S, Mikami H, et al. Retained rice cake: A unique upper gastrointestinal foreign body: Case report and a literature review. Intern Med 2019;58(17):2485–94. [CrossRef]
[Pubmed]
3.
Kopylov U, Nemeth A, Cebrian A, et al. Symptomatic retention of the patency capsule: A multicenter real life case series. Endosc Int Open 2016;4(9):E964–9. [CrossRef]
[Pubmed]
4.
Lin HC, Chen CJ, Lin HH, Huang JT, Chen MJ. Endoscopic treatment of esophageal foreign bodies in the elderly. International Journal of Gerontology 2013;7(1):35–9. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Lim Teik Wen - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yee ZY Francis - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mathur Sachin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Poh RM Benjamin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Lim Teik Wen et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}