 |
Case Report
Deep circumflex iliac artery aneurysm-related retroperitoneal hemorrhage mimicking a ruptured abdominal aortic aneurysm
1 Department of Cardiovascular Surgery, Iizuka Hospital, Fukuoka, Japan
Address correspondence to:
Takashi Matsumoto
MD, Department of Cardiovascular Surgery, Iizuka Hospital, 3-83 Yoshiomachi, Iizuka City, Fukuoka 820-8505,
Japan
Message to Corresponding Author
Article ID: 100148Z12TM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Matsumoto T, Uchida T, Matsuo A, Ishii K, Ando H, Tanaka J. Deep circumflex iliac artery aneurysm-related retroperitoneal hemorrhage mimicking a ruptured abdominal aortic aneurysm. J Case Rep Images Surg 2025;11(1):1–4.ABSTRACT
Introduction: Deep circumflex iliac artery (DCIA) aneurysm is a rare cardiovascular condition whose clinical characteristics are largely unknown. Herein, we report a case of retroperitoneal hematoma caused by a ruptured DCIA aneurysm that mimicked a ruptured abdominal aortic aneurysm (AAA).
Case Report: An 87-year-old woman presented to our hospital with sudden onset of severe abdominal pain. Computed tomography (CT) showed a 58-mm AAA and a marked retroperitoneal hematoma. The patient was diagnosed with ruptured AAA and underwent emergency graft replacement. Owing to the persistent hemorrhage, repeat CT evaluation was performed, which revealed a hemorrhage from an aneurysm in the DCIA. Consequently, coil embolization was performed to achieve hemostasis.
Conclusion: Although DCIA aneurysms are uncommon, the possibility should be considered when diagnosing cases of retroperitoneal hemorrhage, as DCIA yields CT findings and symptoms similar to those of a ruptured AAA.
Keywords: Abdominal aortic aneurysm rupture, Deep circumflex iliac artery, Retroperitoneal hemorrhage
Introduction
Deep circumflex iliac artery (DCIA) aneurysm is a rare cardiovascular condition whose clinical characteristics are largely unknown; consequently, the diagnosis of DCIA is unclear. Deep circumflex iliac artery aneurysms are frequently diagnosed only once they have ruptured and may result in hemorrhage of the abdominal wall, abdominal cavity, or retroperitoneum. Upon rupture, DCIA aneurysms cause abdominal pain and hemodynamic deterioration due to hemorrhaging. Retroperitoneal hemorrhage may manifest without overt signs or symptoms until the degree of hemorrhaging is severe [1]. Furthermore, the differential diagnosis of a DCIA is crucial because its symptoms, such as abdominal pain and clinical imaging presentations, closely resemble those of a ruptured abdominal aortic aneurysm (AAA). Herein, we report a case at our hospital of retroperitoneal hematoma caused by a ruptured DCIA that mimicked a ruptured AAA.
Case Report
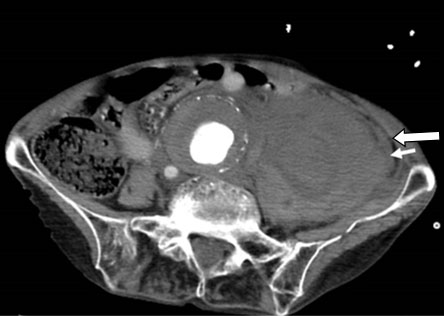
An 87-year-old woman was admitted to our hospital with sudden severe abdominal pain. She had a medical history of hypertension more than 20 years. On examination, she was visibly pale and her systolic blood pressure was 70 mmHg. Blood hemoglobin level had fallen to 8.6 g/L, suggesting the presence of a hemorrhage. Enhanced computed tomography (CT) revealed an abdominal aortic aneurysm with a maximum diameter of 58 mm, accompanied by a retroperitoneal hematoma adjacent to the aneurysm (Figure 1). Computed tomography scan showed no obvious extravasation of contrast medium; however, based on the clinical course, the patient was diagnosed with a retroperitoneal hematoma associated with a ruptured AAA, necessitating emergency surgery. Due to severe tortuosity of the proximal neck below the renal artery, graft replacement was performed rather than stent grafting.
Under general anesthesia, a midline incision was made in the abdomen, which revealed a large retroperitoneal hematoma on the left side of the abdominal aorta with no intraperitoneal hemorrhage. Subsequently, the graft replacement of the AAA was performed based on the anatomy of the patient. Extensive intestinal edema was observed and open abdominal management was performed. Surgery was completed using an open abdominal negative pressure therapy system (ABThera; KCI USA, San Antonio, TX, USA).
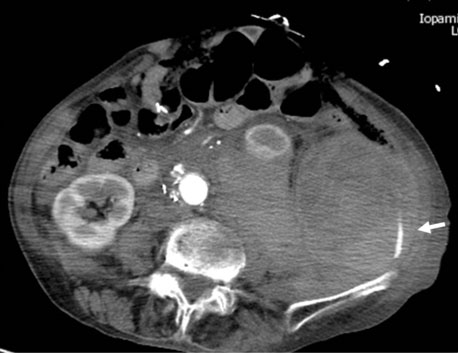
After returning to the intensive care unit, the patient exhibited persistent hemorrhage from the retroperitoneal drain and ABThera. Enhanced CT performed to identify the source of the hemorrhage revealed further enlargement of the retroperitoneal hematoma and extravasation of the contrast medium near the left iliac bone (Figure 2). Emergency interventional radiography was performed.
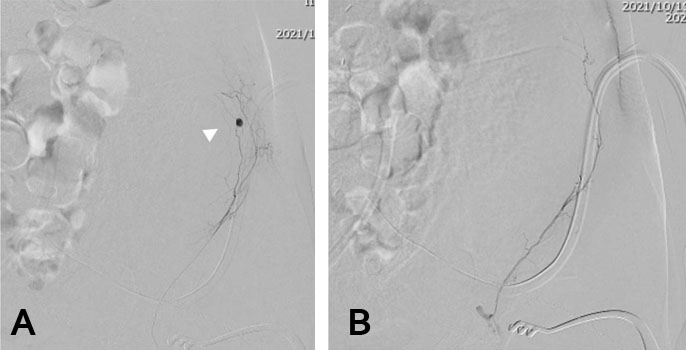
Contrast-enhanced imaging with a sheath inserted through the left femoral artery revealed an arterial aneurysm in the DCIA branching from the left external iliac artery, suggesting that this site was the source of the hemorrhage. A microcatheter was navigated to the site, and coil embolization was performed. Subsequent contrast imaging revealed no residual aneurysm and the procedure was completed after hemostasis was confirmed (Figure 3).
Following hemorrhage control, the patient’s postoperative course was uneventful, and the patient was discharged from the hospital on postoperative day 35.
Discussion
Deep circumflex iliac artery aneurysm is a rare condition, with only nine cases reported to date in the existing literature. Most patients have an iatrogenic false arterial aneurysm, which occurs after undergoing medical procedures such as anterior iliac bone graft harvesting [2], paracentesis [3], post-renal allograft biopsy [4], and laparoscopic inguinal hernia repair [5]. In another case report the diagnosis of a DCIA aneurysm 15 months after kidney transplantation was reported, although there were no specific details in the report [6]. In the present case, no iatrogenic factors were identified. The extensive history of hypertension in this patient and complications of the abdominal aortic aneurysm suggested an arteriosclerotic or idiopathic origin; however, this is only conjecture, as neither a pathological examination of the aneurysm nor a detailed examination of vasculitis was conducted.
The DCIA branches off from the external iliac artery and branches into muscles such as the transverse abdominis, internal abdominal oblique, rectus abdominis, and external abdominal oblique. Thus, the diagnosis of a DCIA aneurysm often relies on the presence of abdominal pain associated with hemorrhage, swelling, and hematoma in the inguinal and lower abdominal areas. However, diagnosing this condition can be challenging in patients who develop a hemorrhage in the retroperitoneal cavity and form a hematoma, as observed in our patient. Patients with abdominal pain due to rupture, hemodynamic deterioration due to hemorrhage, and retroperitoneal hematoma exhibit clinical presentations similar to those with a ruptured AAA. Generally, retroperitoneal hematomas are classified as traumatic or non-traumatic [1]. The most common cause of nontraumatic retroperitoneal hemorrhage is rupture of AAA or aneurysm of other major retroperitoneal blood vessels [7]. In this case, the patient had an AAA with a maximum minor diameter of 58 mm, warranting further treatment. The initial CT evaluation at the time of the hospital visit did not reveal any obvious signs of extravasation from the DCIA, thus adding complexity to the diagnosis. When treating emergency patients presenting with retroperitoneal hematomas, vascular surgeons should consider that ruptured DCIA may mimic the clinical symptoms and CT findings of ruptured abdominal aortic aneurysm.
Embolization of the causative artery has emerged as a highly effective treatment approach for patients with acute hemorrhage, as described in this case report. Loffroy et al. summarized the results of embolization of peripheral false arterial aneurysms in several arteries, including the splenic, carotid, hepatic, superior mesenteric, uterine, and hypogastric arteries [8]. They reported a technical success rate of 100%, successful aneurysm exclusion in 93.8% of the patients, and the absence of complications during an average follow-up of 24.7 months [8]. Another study summarizing the results of paracentesis treatment in 16 patients who developed DCIA or inferior epigastric artery injury reported that although two patients required a second embolization procedure, the treatment of other patients was completed with a single embolization, and all patients survived until hospital discharge [9]. Even in cases where embolization poses a technical challenge, percutaneous thrombin injection into an aneurysm under echocardiographic guidance has been reported to be an effective treatment method [6], warranting consideration.
Conclusion
A retroperitoneal hematoma caused by a ruptured DCIA aneurysm is rare. However, its clinical presentation closely resembles that of abdominal aortic aneurysm rupture, which is a life-threatening condition requiring urgent intervention. Therefore, the differential diagnosis of DCIA aneurysms is important. Vascular surgeons must remain vigilant not only for ruptured arterial aneurysms but also for other conditions that cause retroperitoneal hematoma.
REFERENCES
1.
Mondie C, Maguire NJ, Rentea RM. Retroperitoneal Hematoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
[Pubmed]

2.
Chou ASB, Hung CF, Tseng JH, Pan KT, Yen PS. Pseudoaneurysm of the deep circumflex iliac artery: A rare complication at an anterior iliac bone graft donor site treated by coil embolization. Chang Gung Med J 2002;25(7):480–4.
[Pubmed]
3.
Day RW, Huettl EA, Naidu SG, Eversman WG, Douglas DD, O’Donnell ME. Successful coil embolization of circumflex iliac artery pseudoaneurysms following paracentesis. Vasc Endovascular Surg 2014;48(3):262–6. [CrossRef]
[Pubmed]
4.
Koshy CG, Chacko BR, Babu S, Basu G, Selvaraj D, John GT. An unusual case of abdominal wall bleeding after renal allograft biopsy. Indian J Nephrol 2011;21(1):62–5. [CrossRef]
[Pubmed]
5.
Singh B, Gupta V, Gupta S. Pseudoaneurysm: A complication of laparoscopic inguinal hernia repair. Int J Surg Case Rep 2019;54:39–41. [CrossRef]
[Pubmed]
6.
Fornaro J, Marincek B, Jungius KP. Pseudoaneurysm in the iliac fossa after renal transplantation—treatment with ultrasound-guided thrombin injection. Abdom Imaging 2007;32(1):50–2. [CrossRef]
[Pubmed]
7.
Pode D, Caine M. Spontaneous retroperitoneal hemorrhage. J Urol 1992;147(2):311–8. [CrossRef]
[Pubmed]
8.
Loffroy R, Rao P, Ota S, et al. Packing technique for endovascular coil embolisation of peripheral arterial pseudo-aneurysms with preservation of the parent artery: Safety, efficacy and outcomes. Eur J Vasc Endovasc Surg 2010;40(2):209–15. [CrossRef]
[Pubmed]
9.
Kalantari J, Nashed MH, Smith JC. Post paracentesis deep circumflex iliac artery injury identified at angiography, an underreported complication. CVIR Endovasc 2019;2(1):24. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Takashi Matsumoto - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Takayuki Uchida - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Akinobu Matsuo - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kazuya Ishii - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hiromi Ando - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jiro Tanaka - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AcknowledgmentsWe would like to thank Editage (www.editage.jp) for English language editing
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Takashi Matsumoto et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}