 |
Case Report
Massive pneumoperitoneum and subcutaneous emphysema after transanal resection of a rectal tumor: Case report and comprehensive review of the literature
1 General Surgery, Head of the Department of General Surgery and Digestive System, Hospital Quironsalud Torrevieja, Quironsalud Health Group, Partida de la Loma, S/N, Torrevieja, Alicante 03184, Spain
2 Medical Student, Chicago Medical School, Rosalind Franklin University of Medicine and Sciences, 3333 N Green Bay Rd, North Chicago, IL 60064, USA
Address correspondence to:
Marie Stephanie Nunez Duarte
Chicago Medical School, Rosalind Franklin University of Medicine and Sciences, 3333 N Green Bay Rd, North Chicago, IL 60064,
USA
Message to Corresponding Author
Article ID: 100154Z12PB2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Boix PB, Duarte MSN, Dieter A, Silver R. Massive pneumoperitoneum and subcutaneous emphysema after transanal resection of a rectal tumor: Case report and comprehensive review of the literature. J Case Rep Images Surg 2025;11(1):31–36.ABSTRACT
Introduction: Transanal excision (TAE) is increasingly used to treat malignant polyps and early-stage rectal tumors due to its minimally invasive nature, which facilitates quicker recovery and fewer postoperative complications compared to traditional abdominal approaches. However, while TAE is generally safe, rare complications—such as pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema—can occur, likely related to insufflation pressures during the procedure.
Case Report: We report the case of a 72-year-old woman who underwent TAE for a rectal adenocarcinoma. The procedure was completed without evidence of intraoperative perforation. Nonetheless, on postoperative day one, the patient developed respiratory distress, fever, and abdominal discomfort. Imaging studies revealed the presence of air in the retroperitoneum and soft tissues. She was managed conservatively with intravenous antibiotics and supportive care, leading to full recovery by day four without the need for additional surgical intervention.
Conclusion: This case underscores that, although TAE offers significant benefits in terms of reduced morbidity, clinicians should remain vigilant for rare but dramatic complications. In the absence of peritonitis or sepsis, conservative management appears effective, supporting the continued use of TAE as a safe and minimally invasive option for rectal tumor excision.
Keywords: Pneumoperitoneum, Pneumoretroperitoneum, Rectal adenocarcinoma, Subcutaneous emphysema, Transanal excision
Introduction
Colorectal cancer is the second most commonly diagnosed cancer in both men and women in the United States, with colon polyps being a common precursor [1],[2],[3]. While many polyps are benign, those with cancerous cells penetrating the muscularis mucosae are classified as malignant polyps, categorized as T1NxMx in the TNM staging system. Transanal excision (TAE) is a minimally invasive treatment for select low rectal cancers, offering quicker recovery and fewer postoperative complications compared to traditional surgical approaches [3]. However, complications such as bleeding, perforation, infection, and stricture may occur, with rare cases of pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema also reported. These rare complications are believed to stem from insufflation pressures during surgery, which can allow air to track through tissue planes and highlight the complex anatomical continuity between the retroperitoneal, mediastinal, and subcutaneous spaces.
Understanding these mechanisms is vital as they often present with dramatic radiological findings but resolve with conservative management, avoiding the need for surgical intervention. This report describes a rare case of pneumoperitoneum, pneumoretroperitoneum, and emphysema following TAE for a rectal tumor, while exploring the clinical implications and management strategies based on a review of the literature.
Case Report
A 72-year-old woman with a positive fecal occult blood test underwent a colonoscopy, which identified a 1 cm flat lesion located 5 cm from the anal margin. An en-bloc mucosectomy was performed. Histopathological analysis revealed a tubular adenoma with moderate epithelial dysplasia and a focus of moderately differentiated infiltrating adenocarcinoma extending beyond the muscularis layer into the submucosa, with an artifacted margin at 1.1 mm. Preoperative imaging, including computed tomography (CT) of the chest, abdomen, and pelvis, as well as pelvic magnetic resonance imaging (MRI) showed no significant alterations.
The patient subsequently underwent a transanal full-thickness resection using an ultrasonic scalpel (harmonic). Intraoperative rectoscopy up to 25 cm confirmed the site of the previous polypectomy scar, located on the posterior rectal wall, 5 cm from the anal verge. No tumor was detected on digital rectal examination. The excision encompassed the entire rectal wall, and the defect was closed using a running absorbable V-Loc suture. No peritoneal breach or intraoperative perforation was observed.
On postoperative day one, the patient became drowsy and developed dyspnea, fever, and abdominal discomfort. A CT scan revealed pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema extending to the cervical and thoracic regions. She was transferred to the Intensive Care Unit (ICU) for 48 hours of close monitoring. Conservative management with intravenous meropenem (800 mg every 8 hours) and teicoplanin (400 mg every 12 hours) was initiated, along with analgesic therapy.
The patient remained hemodynamically stable throughout her ICU stay, with gradual resolution of the emphysema. She was subsequently transferred to a general ward, and by postoperative day four, all symptoms had resolved. She was discharged home on oral antibiotics without complications. Postoperative histopathological examination of the resected specimen confirmed the absence of residual neoplastic tissue. The final diagnosis for the patient was pneumoperitoneum and subcutaneous emphysema after transanal excision of a rectal adenocarcinoma, without evidence of peritoneal perforation or residual malignancy.
Discussion
Transanal excision of rectal polyps is a minimally invasive procedure widely used to treat colorectal cancer in the distal rectum. Compared to open surgical approaches, TAE is associated with fewer postoperative complications, such as bleeding, pelvic sepsis, urinary retention, suture dehiscence, and fecal incontinence [4],[5]. Despite its overall safety, rare complications like pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema have been reported in the literature. A review of 13 studies, shown in Table 1, identified 17 cases involving these rare complications following full-thickness rectal wall resections [6],[7],[8],[9],[10],[11],[12]. These complications represent a small subset of the adverse events associated with these generally low-risk techniques, which include endoscopic microsurgery (TEM) and transanal resection. Except for one case requiring surgical intervention involving a loop colostomy, all patients recovered fully with conservative management [13]. In other cases, management included antibiotics and close monitoring, with no long-term sequelae.
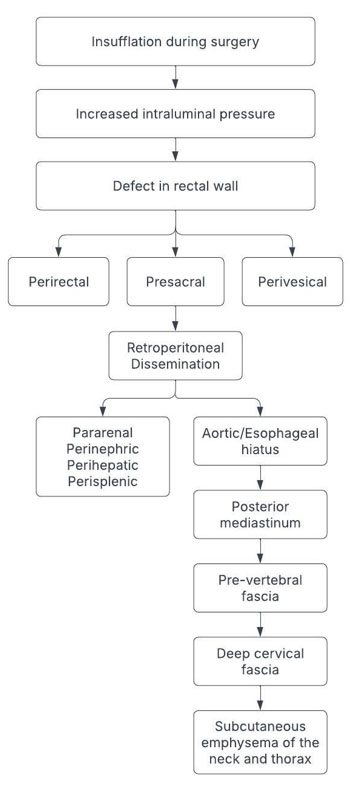
The mechanisms underlying these complications are thought to involve insufflation pressures during surgery, leading to air diffusion along tissue planes. The complete dissemination route is illustrated in Figure 1. During transanal excision, insufflation of CO2 or room air into the rectal lumen is used to enhance visualization, increasing intraluminal pressure. Pressure can force air into adjacent tissue planes during full-thickness resection. Even without a peritoneal breach, air may escape and follow natural anatomical pathways. It accumulates in the perirectal space, then spreads posteriorly to the presacral space and anteriorly to the perivesical region. Air may then ascend through retroperitoneal fascial planes, reaching the perihepatic, perisplenic, pararenal, and perinephric areas. It tracks into the posterior mediastinum via the aortic or esophageal hiatus, dissecting cranially along major vascular structures. From the mediastinum, air moves superiorly through the prevertebral fascial planes and disseminates along the deep cervical fascia. This results in subcutaneous emphysema of the neck and thorax, with potential extension to the face and scalp in more severe cases. While radiologically striking, these patterns usually resolve with antibiotics, monitoring, and supportive care. Surgery is only necessary if clinical deterioration or peritonitis occurs.
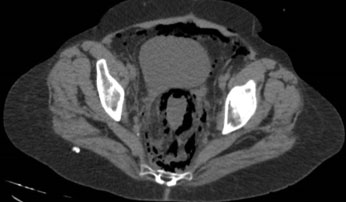
This proposed pathway is supported by both anatomical continuity and clinical imaging findings. Peritoneal rupture was not observed in any of the reported cases, including the present one. Instead, insufflation of CO2 or room air likely contributed to air dissemination, particularly when coupled with reduced tissue integrity following full-thickness resections [14],[15]. This hypothesis aligns with the findings in Figure 2 and Figure 3 of this case report, which demonstrate the extensive presence of gas in the perihepatic, perisplenic, presacral, perirectal, perivesical, and retroperitoneal spaces. These findings highlight the anatomical continuity between retroperitoneal, mediastinal, and subcutaneous spaces, providing a clear pathway for air to traverse without requiring direct peritoneal breach [16],[17]. Similar imaging patterns have been observed in other reports, such as the cases described by Chandra in 2014, where insufflation led to intraoperative hypercarbia, which resolved spontaneously without additional intervention.
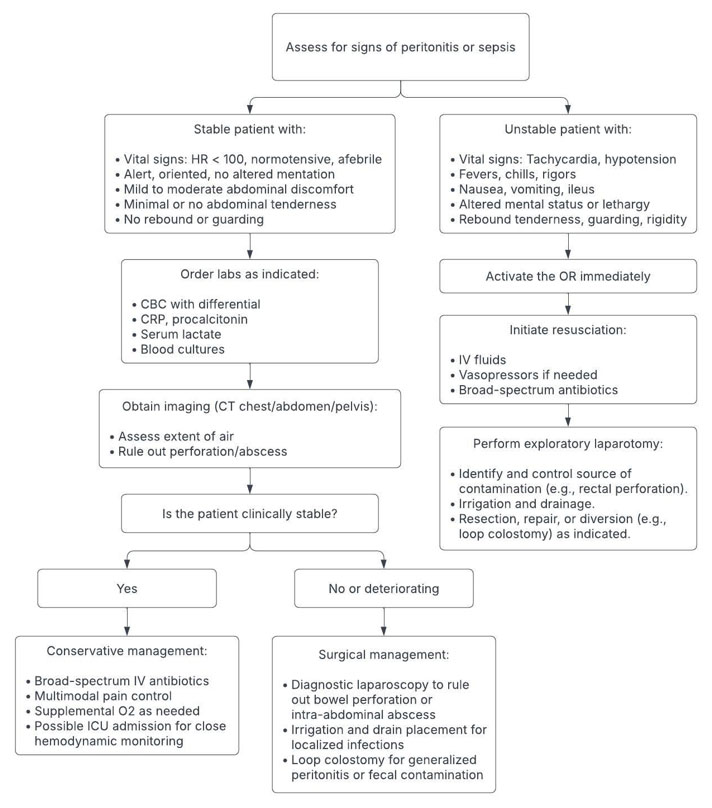
Management of pneumoperitoneum and subcutaneous emphysema following transanal excision is largely dictated by the patient’s clinical stability. Patients who are hemodynamically stable, without signs of peritonitis or systemic infection, and who have reassuring labs and imaging, can be safely managed with intravenous antibiotics, supportive care, and close monitoring. However, the presence of hemodynamic instability, fever, leukocytosis, elevated lactate, or imaging findings suggestive of bowel perforation or abscess warrants immediate surgical evaluation. Operative intervention may involve diagnostic laparoscopy, repair of a defect, drainage of localized infection, or fecal diversion if contamination is extensive. This stepwise clinical decision-making process is outlined in Figure 4, which serves as a practical reference for triaging patients with these rare but potentially serious postoperative complications. Prompt recognition and appropriate escalation are critical to optimizing outcomes while avoiding unnecessary surgical intervention.
As severe complications remain exceedingly rare, these findings should not dissuade the use of TAE or TEM as safe and effective approaches for rectal tumor excision. The observed radiological findings, while dramatic, typically resolve with conservative management in the absence of sepsis or peritonitis. Surgical intervention should remain a last resort, reserved for cases with significant clinical deterioration, which remains exceedingly rare. The current case and supporting literature emphasize that close observation, antibiotic therapy, and dietary restrictions, when indicated, are sufficient to manage these complications effectively while ensuring favorable outcomes. Long-term outcomes are less clear due to lack of reporting in the literature; however, all but one patient had nearly complete resolution of their symptoms at their postoperative evaluations within a month after the surgery. Only one complication—a loop colostomy due to sepsis—required long-term follow-up, and it was successfully reversed six months later. This supports the continued use of TAE as a safe and minimally invasive approach for rectal tumor management.


Conclusion
Transanal excision of rectal polyps is a minimally invasive procedure that has demonstrated fewer postoperative complications compared to open surgical approaches, making it a widely adopted technique for treating distal colorectal cancer. Common complications such as bleeding, pelvic sepsis, urinary retention, and suture dehiscence are well documented. However, rare complications like pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema have been reported in a small number of cases.
In these cases, understanding the anatomical pattern of air dissemination is essential for guiding diagnosis and management. We describe this pattern of spread from the rectum through retroperitoneal, mediastinal, and subcutaneous planes in our discussion. We have documented the findings of air dissemination radiographically in our case, with gas seen in the perihepatic, perisplenic, presacral, perirectal, perivesical, and retroperitoneal spaces. Closely mirror prior reports and support the role of insufflation pressure, rather than gross perforation, as the primary mechanism of spread. Our review of the literature reveals that these complications have been documented in ten studies involving fourteen patients, all of whom underwent full-thickness rectal wall resections using techniques like transanal endoscopic microsurgery (TEM) or transanal resection. Except for one case requiring surgical intervention with a loop colostomy, all other cases resolved with conservative management, indicating the typically benign nature of these events. Lastly, to aid in determining when surgery is warranted, We have presented a structured management algorithm based on patient stability, physical exam findings, and radiologic patterns. This guidance may help clinicians recognize when conservative care is appropriate and avoid unnecessary operative intervention.
REFERENCES
1.
Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin 2023;73(3):233–54. [CrossRef]
[Pubmed]

2.
Cowan ML, Silviera ML. Management of rectal polyps. Clin Colon Rectal Surg 2016;29(4):315–20. [CrossRef]
[Pubmed]
3.
Léonard D, Remue C, Kartheuser A. The transanal endoscopic microsurgery procedure: Standards and extended indications. Dig Dis 2012;30 Suppl 2:85–90. [CrossRef]
[Pubmed]
4.
Bignell MB, Ramwell A, Evans JR, Dastur N, Simson JNL. Complications of transanal endoscopic microsurgery (TEMS): A prospective audit. Colorectal Dis 2010;12(7 Online):e99–103. [CrossRef]
[Pubmed]
5.
Shaltiel T, Gingold-Belfer R, Kirshtein B, Issa N. The outcome of local excision of large rectal polyps by transanal endoscopic microsurgery. J Minim Access Surg 2023;19(2):282–7. [CrossRef]
[Pubmed]
6.
Bonardi RA, Rosin JD, Witkin E. Subcutaneous emphysema, pneumoretroperitoneum, and pneumomediastinum following rectal surgery: Report of a case and review of the literature. Dis Colon Rectum 1976;19(8):710–2. [CrossRef]
[Pubmed]
7.
Kriss BD, Porter JA, Slezak FA. Retroperitoneal air after routine hemorrhoidectomy. Report of a case. Dis Colon Rectum 1990;33(11):971–3. [CrossRef]
[Pubmed]
8.
Petros JG, Thanikachalam M, Lopez MJ. Retroperitoneal and abdominal wall emphysema after transanal excision of a rectal carcinoma. Am Surg 1996;62(9):759–61.
[Pubmed]
9.
Cantos M, Bruna M, García-Coret MJ, Villalba FL, Roig JV. Pneumomediastinum and subcutaneous emphysema like strange complications after transanal endoscopic microsurgery. [Article in Spanish]. Rev Esp Enferm Dig 2009;101(6):445–6. [CrossRef]
[Pubmed]
10.
Sato K, Itoh S, Shigiyama F, Kitagawa T, Maetani I. Pneumoretroperitoneum, pneumomediastinum and subcutaneous emphysema after colorectal endoscopic submucosal dissection (ESD) with air insufflation. J Interv Gastroenterol 2011;1(3):136–8. [CrossRef]
[Pubmed]
11.
Liang HH, Tu CC, Hung CS, Wei PL, Yen KL, Kuo LJ. “Air bubble” in the head after transanal excision of a rectal carcinoma. J Emerg Med 2013;44(2):e273–4. [CrossRef]
[Pubmed]
12.
Simkens GA, Nienhuijs SW, Luyer MD, de Hingh IH. Massive surgical emphysema following transanal endoscopic microsurgery. World J Gastrointest Surg 2014;6(8):160–3. [CrossRef]
[Pubmed]
13.
Martins BAA, Coura MMA, de Almeida RM, Moreira NM, de Sousa JB, de Oliveira PG. Pneumoretroperitoneum and sepsis after transanal endoscopic resection of a rectal lateral spreading tumor. Ann Coloproctol 2017;33(3):115–8. [CrossRef]
[Pubmed]
14.
Chandra A, Clarke R, Shawkat H. Intraoperative hypercarbia and massive surgical emphysema secondary to transanal endoscopic microsurgery (TEMS). BMJ Case Rep 2014;2014:bcr2013202864. [CrossRef]
[Pubmed]
15.
Franken RJ, Moes DE, Acherman YIZ, Derksen EJ. Free intra-abdominal air without peritoneal perforation after TEM: A report of two cases. Case Rep Surg 2012;2012:185429. [CrossRef]
[Pubmed]
16.
Farmer KC, Tjandra JJ, Hockenberry S, Fazio VW. Pneumomediastinum following transanal excision of a rectal tumour. Aust N Z J Surg 1993;63(7):568–71. [CrossRef]
[Pubmed]
17.
Sunderland MS, Dakwar A, Rishi A, Bennett RD. Pneumoperitoneum, pneumoretroperitoneum, and pneumoscrotum following transanal excision of rectal polyp. Am Surg 2023;89(4):1107–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
P Bretcha Boix - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Marie Stephanie Nunez Duarte - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
A Dieter - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
R Silver - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Bretcha Boix et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}