 |
Case Report
Choledocholithiasis as a cause of spontaneous common bile duct perforation: From myths to reality. A case report
1 Clinician, Resident in General Surgery, Pontificia Bolivariana University, Medellín, Colombia
2 Clinician, Specialist in General Surgery, Pablo Tobón Uribe Hospital, Medellín, Colombia
3 Clinician, Specialist in General Surgery and Hepatobiliary Surgery, Pablo Tobón Uribe Hospital, Medellín, Colombia; Hepatobiliary and Liver Transplant Program, Pablo Tobón Uribe Hospital, University of Antioquia, Medellín, Colombia
4 Hepatobiliary and Liver Transplant Program, Pablo Tobón Uribe Hospital, University of Antioquia, Medellín, Colombia
5 Gastrohepatology Research Group, University of Antioquia, Medellín, Colombia
Address correspondence to:
Camila Arias González
Resident in General Surgery, Pontificia Bolivariana University, Medellín,
Colombia
Message to Corresponding Author
Article ID: 100156Z12CG2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
González CA, Gómez PMJ, Ospina DAG, Garcés ÁAD, Duque SIH. Choledocholithiasis as a cause of spontaneous common bile duct perforation: From myths to reality. A case report. J Case Rep Images Surg 2025;11(1):42–46.ABSTRACT
Introduction: Spontaneous common bile duct (CBD) perforation is a rare complication of choledocholithiasis. Typically, it is diagnosed during surgery, particularly exploratory laparotomy, in patients experiencing acute abdomen.
Case Report: We present a case of a 16-year-old female with no prior medical history except for a cesarean section two months prior, who presented to the emergency department with abdominal pain. During surgery, we diagnosed spontaneous common bile duct (CBD) perforation due to choledocholithiasis and described the treatment.
Conclusion: Due to its low incidence, diagnosis of spontaneous CBD perforation is often delayed, leading to increased morbidity and mortality. Symptoms vary, and diagnostic imaging is nonspecific. Treatment choice between conservative and surgical approaches depends on patient hemodynamic stability, perforation characteristics, and CBD condition. Surgical options include bile duct repair or reconstruction. Spontaneous CBD perforation is rare and usually diagnosed during surgery. Treatment ranges from conservative measures to bile duct reconstruction.
Keywords: Choledocholithiasis, Common bile duct, Spontaneous perforation
Introduction
Perforations of the biliary system mainly occur in the gallbladder and are associated with acute cholecystitis. Spontaneous CBD perforation is uncommon, standing for just 10% of biliary tract perforations. It is primarily described in children, often associated with congenital anomalies of the biliary system. In adults and pregnant women, the cause is mostly idiopathic; however, it may occur as a complication of choledocholithiasis [1]. This phenomenon seems to be related to intramural infections, ischemic bile duct necrosis, an increase in intraductal pressure, or erosion of the duct caused directly by a gallstone [2],[3].
Due to the low incidence of spontaneous CBD perforations, this pathology is not usually suspected, and the diagnosis is rarely made in the preoperative setting. In most cases, the perforation is first evident during an exploratory laparotomy, posing a challenge on treatment due to the lack of presurgical planning [4].
We describe the case and treatment of a female patient without previous illnesses, who presented with spontaneous CBD perforation caused by choledocholithiasis. During our literature review, we found little information among different databases, probably due to the low prevalence of this complication. In the current literature on this topic, there are only a few case reports available. This is the first case of spontaneous CBD perforation reported in Latin America.
Case Report
A 16-year-old female, without previous illnesses, endoscopic procedures, or surgical interventions, besides a C-section two months prior, presented to the emergency department of a tertiary care hospital with abdominal pain, initially in the epigastrium and later generalized. An abdominal ultrasound showed inflammatory changes in the right flank and right iliac fossa, consistent with a thick fluid collection of 296 mL, with no distended gallbladder or dilatation of the intrahepatic biliary duct. The appendix could not be visualized by this method. A ruptured appendix, as the most probable diagnosis, was considered, and a laparotomy was performed. During the procedure, a large amount of turbid fluid was found, along with a plastron at the level of the hepatic angle of the colon. The appendix had a macroscopic normal appearance without signs of inflammation. Since no other origin for the pain was found, an appendectomy was performed, and abdominal drainage was inserted at the right flank.
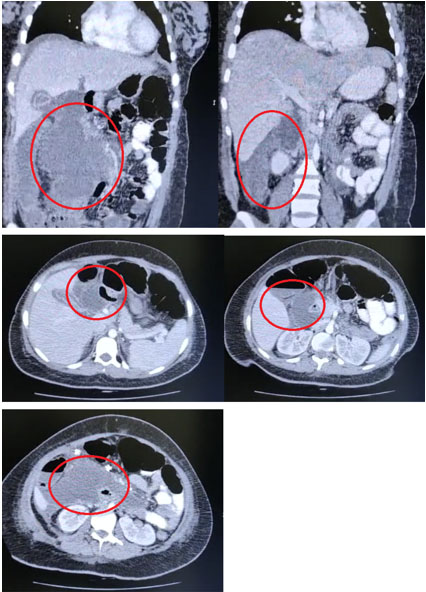
The patient continued to experience abdominal pain in the postoperative period. She presented with persistent tachycardia and a greenish-yellow fluid in the drainage, prompting an abdominal tomography on the second day after surgery (Figure 1), revealing free fluid and collections between the intestinal loops without hepatic lesions or other alterations. The surgeons decided to perform another laparotomy, revealing biliary peritonitis of the four quadrants without alterations in the gallbladder or bile duct. The intestine was intact; however, bile seemed to originate from the hepatic hilum with no apparent source. Subsequently, a subhepatic drainage was inserted, and the patient was transferred to a higher care hospital for further diagnostic workup.
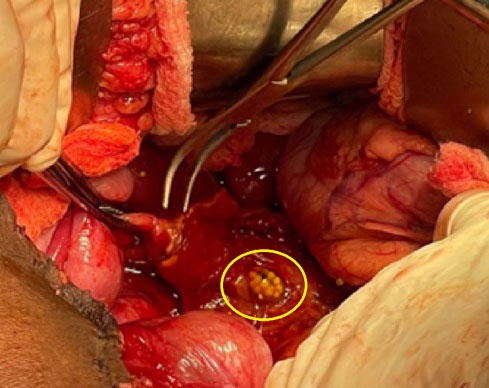
The patient arrived at the quaternary care hospital in poor condition, tachycardic, with fever, and signs of peritoneal irritation. Liver function was normal, with a C-reactive protein of 7.7 mg/dL, leukocytes of 10,700 mm3, and platelets of 512,000 mm3. An urgent exploratory laparotomy was planned due to suspected duodenal perforation. The surgery revealed free serous intrabdominal fluid, adhesions of the small intestine to the pelvis, a long appendiceal stump, inflammatory changes in the right retroperitoneum, and distal CBD necrosis with a secondary perforation due to an embedded gallstone, as observed in Figure 2. The gallbladder had a normal macroscopic aspect. Drainage of the peritonitis and release of the right colon through Toldt’s line and Kocher’s maneuver were performed to achieve adequate exposure of the duodenum and hepatic hilum, which showed a significant inflammatory process. Support from hepatobiliary surgery was requested during the intraoperative period, and a careful cholecystectomy was performed. Due to the condition of the bile duct, it was not possible to perform a primary raffia or management with a T-tube. Therefore, a distal bile duct resection and reconstruction with Roux-en-Y hepaticojejunostomy were opted for.
In the following days, the patient showed good clinical evolution with normal liver function and decreasing acute phase reactants. Escherichia coli with intermediate resistance to beta-lactamases was isolated in the peritoneal fluid cultures, and antibiotic management with meropenem was started for seven days. Discharge was conducted without complications.
Discussion
The spontaneous CBD perforation is an uncommon entity, which may occur as a complication of choledocholithiasis. It was first described in 1882 by Freeland, who reported this pathology when he found multiple diverticula surrounding the CBD with gallstones during an autopsy [5]. After this first report, only a few cases have been reported due to its low incidence. Most cases have been described in children due to congenital anomalies of the biliopancreatic system [2],[4]. In the general adult population, it is extremely rare. The largest case series of spontaneous CBD perforation was published by Chu in 1984 with 4 cases and by Kang in 2004 with 11 cases [6]. There have been only a few cases in pregnant women, the first one reported by Piotrowski in 1900 [7].
Because of a CBD perforation, biliary peritonitis can occur, which can also be caused by perforations in other more frequent places such as the gallbladder (91% of the cases), cystic duct (3.3%), or the superior gastrointestinal tract [3],[8].
The main cause of CBD perforation is iatrogenic, usually after procedures such as endoscopic retrograde cholangiopancreatography (ERCP) or cholecystectomy. In the case of spontaneous CBD perforation in adults, the main cause remains idiopathic [3]. Nevertheless, two theories have been suggested to explain the pathogenesis. On one hand, the perforation can result from the weakness and necrosis of the CBD wall, probably due to CBD cysts, pancreatitis, chronic infections, ischemia, biliopancreatic reflux, torsion of the gallbladder, or erosion of the wall caused by a gallstone directly [2]. On the other hand, an increase in intraductal pressure due to choledocholithiasis, congenital stenosis of the ampulla of Vater, Oddi’s sphincter spasms, or the presence of parasites in the CBD may also play a key role [9],[10].
In general, the presurgical diagnosis of a spontaneous CBD perforation is particularly challenging and is usually made during surgery because patients present with a variety of signs and symptoms that are not specific or suggest other more common entities [4]. This happened in our case, where the first presumptive diagnosis was acute appendicitis, and even with the presence of biliary fluid in the abdominal cavity, CBD perforation was not suspected. Additionally, abdominal imaging showed neither biliary pathology nor dilatation of the biliary system, and hepatic function was consistently normal, making the real diagnosis even harder to establish.
Most of the reported cases in the literature presented with symptoms such as progressive jaundice, painless abdominal distension, and acholia, but up to 20% of the patients showed more serious symptoms such as fever, peritoneal irritation, and hemodynamic instability [9]. Thus, the severity of symptoms may vary from diffuse pain in the right hypochondrium to threatening generalized peritonitis [4].
In abdominal computed tomography or ultrasound, indirect signs of a CBD perforation can be seen, such as a compressed gallbladder (empty gallbladder), perihepatic collections, or intra-abdominal free fluid. However, in most cases, there is no evidence of the exact perforation site. In some case series, the presurgical diagnosis was set up with magnetic resonance cholangiopancreatography or ERCP [11],[12]. Retrospectively, we found in our case the aforementioned tomographic signs. However, these signs are not specific for a CBD perforation, and due to the low incidence of spontaneous CBD perforations, the diagnosis was not made or even suspected in the presurgical setting.
Other methods, such as scintigraphy, may more precisely show the site of perforation, but this method is not routinely used in our community [9]. Another diagnostic tool is abdominal paracentesis, which in this case would reveal bile in the peritoneal fluid. Nonetheless, this finding is more often found in perforations of the gallbladder due to gangrenous cholecystitis.
The aim of surgical treatment is to stop the bile leak and correct choledocholithiasis and cholangitis if present. Then, the need for biliary tract reconstruction must be decided [13].
The approach in the intraoperative period depends on several aspects. In hemodynamically stable patients or those without signs of generalized peritonitis, conservative treatment can be performed, similar to patients with iatrogenic lesions of the bile duct, where it is possible to manage them with ERCP and biliary stent placement in combination with percutaneous drainage [4]. On the other hand, in patients who fulfil criteria for surgical management, ideally, preoperative cholangiography should be performed, and in the case of showing no obstruction distal to the perforation, an exploration of the bile duct and a primary closure of the perforation can be conducted. Generally, the procedure consists of T-tube insertion and cholecystectomy [4],[9],[13]. In the case of obstruction distal to the perforation, primary repair is not possible. In this scenario, it is indicated to perform bile duct reconstruction with a Roux-en-Y hepaticojejunostomy [9]. Drain insertion is crucial in these cases to ensure adequate drainage of the abdomen [13].
In our case, the patient had necrosis of the CBD wall in addition to the perforation, which was diagnosed during an emergency laparotomy due to an acute abdomen, without suspecting that the cause of the peritonitis was a CBD perforation. Due to these conditions, the management that we considered most appropriate was the reconstruction of the bile duct with Roux-en-Y hepaticojejunostomy with the support of hepatobiliary surgery, which is the ideal specialty to perform this type of reconstruction, especially in our patient who had a bile duct without dilatation, making the bilioenteric shunt a much more complex procedure. With this management, we were able to obtain good immediate post-surgical results in the patient.
Conclusion
Spontaneous CBD perforation is a rare entity that may be present as a complication of choledocholithiasis. In most cases, the preoperative diagnosis is difficult to establish, and there is currently no gold standard imaging modality. The treatment of this pathology depends on several aspects and varies from a conservative approach, such as an ERCP with stent placement, to the need to perform a reconstruction of the bile duct, depending on the hemodynamic status of the patient and the anatomical characteristics of the perforation.
REFERENCES
1.
Dabbas N, Abdelaziz M, Hamdan K, Stedman B, Abu Hilal M. Gallstone-induced perforation of the common bile duct in pregnancy. HPB Surg 2008;2008:174202. [CrossRef]
[Pubmed]

2.
Subasinghe D, Don Udayakumara EA, Somathilaka U, Huruggamuwa M. Spontaneous perforation of common bile duct: A rare presentation of gall stones disease. Case Rep Gastrointest Med 2016;2016:5321304. [CrossRef]
[Pubmed]
3.
Hamura R, Haruki K, Tsutsumi J, Takayama S, Shiba H, Yanaga K. Spontaneous biliary peritonitis with common bile duct stones: Report of a case. Surg Case Rep 2016;2(1):103. [CrossRef]
[Pubmed]
4.
Bouzid A, Fendri S, Rejab H, Trigui A, Mejdoub Y, Boujelbene S. Spontaneous perforation of the common bile duct in adults presenting as biliary peritonitis: A case report and literature review. Ann Med Surg (Lond) 2023;85(3):460–5. [CrossRef]
[Pubmed]
5.
Freeland J. Rupture of the hepatic duct. Lancet 1882;119(3062):731–2.
6.
Gkionis IG, Flamourakis ME, Strehle AF, et al. A Rare case of extended retroperitoneal biloma due to spontaneous perforation of common bile duct, mimicking a strangulated right inguinal hernia: A case report and literature review. Am J Case Rep 2022;23:e936255 [CrossRef]
[Pubmed]
7.
Piotrowski JJ, Van Stiegmann G, Liechty RD. Spontaneous bile duct rupture in pregnancy. HPB Surg 1990;2(3):205–9. [CrossRef]
[Pubmed]
8.
Masroor M, Sarwari MA. Spontaneous common bile duct perforation in full term pregnancy: A rare case report and review of literature. BMC Surg 2021;21(1):239. [CrossRef]
[Pubmed]
9.
Mohanty SK, Mahapatra T, Behera BK, et al. Spontaneous perforation of common bile duct in a young female: An intra-operative surprise. Int J Surg Case Rep 2017;35:17–20. [CrossRef]
[Pubmed]
10.
Sakamoto R, Kai K, Hiyoshi M, et al. Spontaneous common bile duct perforation due to choledocolithiasis accompanied with pancreaticobiliary maljunction in an adult: A case report. Surg Case Rep 2021;7(1):205. [CrossRef]
[Pubmed]
11.
Amberger M, Burton N, Tissera G, Baltazar G, Palmer S. Spontaneous common bile duct perforation—A rare clinical entity. Int J Surg Case Rep 2018;46:34–7. [CrossRef]
[Pubmed]
12.
Pülat H, Karaköse O, Benzin MF, Sabuncuoğlu MZ, Çetin R. A rare cause of acute abdomen: Spontaneous common hepatic duct perforation. Ulus Travma Acil Cerrahi Derg 2016;22(1):103–5. [CrossRef]
[Pubmed]
13.
Mizutani S, Yagi A, Watanabe M, et al. T tube drainage for spontaneous perforation of the extrahepatic bile duct. Med Sci Monit 2011;17(1):CS8–11. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Camila Arias González - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Paula María Jaramillo Gómez - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
David Alejandro González Ospina - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Álvaro Andrés Duarte Garcés - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sergio Iván Hoyos Duque - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Camila Arias González et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}