 |
Case Report
Twin-Stone syndrome: A rare presentation of gallstone ileus
1 Department of Surgery, Cooper University Hospital, Camden, NJ, USA
2 Cooper Medical School of Rowan University, Camden, NJ, USA
Address correspondence to:
T N Hess
3 Cooper Plaza, Suite 411, Camden, NJ 08103,
USA
Message to Corresponding Author
Article ID: 100160Z12TH2025
Access full text article on other devices

Access PDF of article on other devices

How to cite this article
Hess TN, Brigando ON, Bailey DW. Twin-Stone syndrome: A rare presentation of gallstone ileus. J Case Rep Images Surg 2025;11(2):10–13.ABSTRACT
Introduction: Gallstone ileus is a rare cause of mechanical bowel obstruction resulting from gallstone migration through a cholecystoenteric fistula, most commonly impacting the ileocecal valve. Bouveret syndrome, a rare variant, involves gastric outlet obstruction from proximal impaction.
Case Report: We present the case of a 61-year-old female with a closed-loop obstruction caused by multiple impacted gallstones. Surgical management for this patient included enterotomy, cholecystectomy, pyloroplasty, common bile duct resection with hepaticojejunostomy, and closure of the cholecystoduodenal fistula. The patient recovered well with a short episode of post-operative atrial fibrillation.
Conclusion: This case of Twin-Stone syndrome highlights the complexity of treating gallstone ileus, particularly with more complicated sites of obstruction combined with fistula formation. Surgical management of this complex disease should be tailored to the patient’s clinical scenario to provide optimal outcomes in this high-risk population.
Keywords: Acute care surgery, Gallstone ileus, Small bowel obstruction
Introduction
Gallstone ileus is a complication of cholelithiasis, with an incidence ranging from 0.3% to 1.5%, and accounts for 1–5% of all cases of mechanical bowel obstruction [1]. It occurs when an impacted gallstone migrates into the gastrointestinal tract through a cholecystoenteric fistula. These fistulas can develop along the gastrointestinal tract including the duodenum and stomach. Gallstones can cause obstruction at several points along the gastrointestinal tract, with the most frequent site being the ileocecal valve (50–70%), followed by the sigmoid colon, ligament of Treitz, and second portion of the duodenum [2].
Similarly, Bouveret syndrome is a rare variant of gallstone ileus that accounts for approximately 2–3% of all cases of gallstone-related obstructions and occurs when the gallstone causes gastric outlet obstruction [3]. Both variants of gallstone ileus present with a variety of symptoms, including nausea, vomiting, and abdominal pain. Diagnosis is made radiographically with the hallmark finding of Rigler’s triad, characterized by pneumobilia, bowel dilation with a transition point, and an ectopic gallstone.
Gallstone ileus and Bouveret syndrome are associated with substantial morbidity and mortality. Previous studies report the in-hospital mortality for gastrointestinal (GI) to be 6.7%, and the most common complication was acute renal failure, which occurred in 30% of cases [1]. Management is guided by the location and size of the obstructing gallstone, with treatment strategies including either surgical extraction or, in select cases, endoscopic retrieval. Here we present a patient with a closed-loop obstruction caused by two separate impacted gallstones. This is a surgical emergency as the two points of obstruction increase the risk of ischemia and perforation for the closed-off portion of the intestine.
Case Report
Presentation: A 61-year-old female with a past medical history of breast cancer, cervical dysplasia, hyperlipidemia, and pulmonary thromboembolism presented to the emergency department with four days of right-sided abdominal pain and two days of emesis. She underwent cholecystectomy at a separate facility that was aborted due to extensive adhesions and the discovery of a cholecystoduodenal fistula. A drain was placed and she was transferred to a tertiary care center. On arrival, she was tachycardic to the 110 s and blood pressure was 112/82 mmHg. Her labs were notable for a white blood cell count of 14.60 × 103/μL.
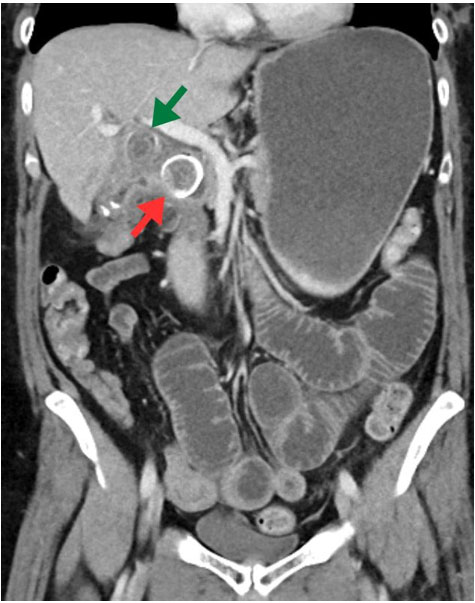
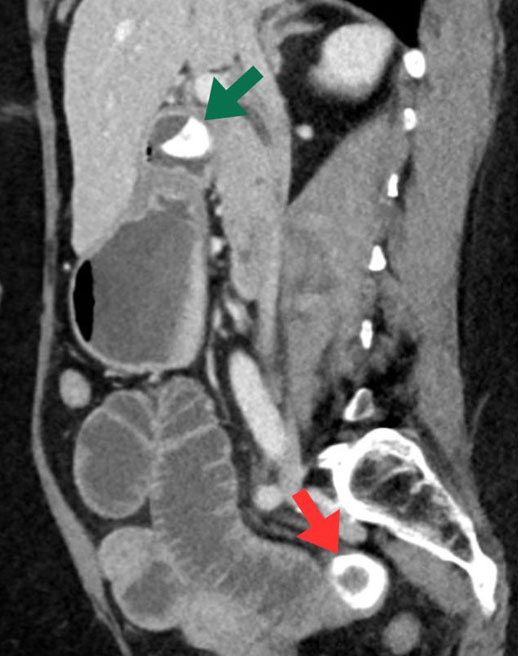
Imaging: Diagnosis was confirmed on computed tomography (CT) of abdomen and pelvis, which revealed a 2.5 cm intraluminal gallstone within the pylorus causing a partial obstruction (Figure 1) and dilated loops of small bowel in the posterior pelvis secondary to a 2.8 cm calcified gallstone in the distal jejunum (Figure 2).
Management: Due to her closed-loop obstructive symptoms, she underwent an exploratory laparotomy which revealed significant adhesions within the right upper quadrant. As her bowel was inspected, there were no areas of ischemia and a 4-cm stone was identified within the jejunum with proximal dilation and distal decompressed loops representing a transition point. A longitudinal enterotomy was performed, and the stone was removed. This was then closed transversely in 2 layers. Proximally, a stone was identified within the pylorus and a second stone within the common bile duct. At this time, due to the complex nature of the case and the need for reconstruction at the index operation, surgical oncology was called to assist. A top-down approach was used to perform a cholecystectomy, and the cystic duct was identified and fused to the common bile duct. An open common bile duct exploration was performed, and the stone was removed. Due to the extent of inflammation and fibrosis, the common bile duct was resected. Next, attention was turned to the stomach. A pyloromyotomy was performed to remove the impacted stone and was closed via a Heineke–Mikulicz pyloroplasty. Finally, a retrocolic Roux-en-Y hepaticojejunostomy was performed to reconnect the biliary system and the duodenal fistula tract was closed and buttressed with a jejunal patch.
Outcome: A nasogastric tube was left in place for decompression for five days, when she underwent an upper gastrointestinal series to ensure no ongoing leak. Her only post-operative complication was atrial fibrillation, which was easily controlled. The patient underwent a fluoroscopic upper gastrointestinal series with water-soluble contrast, which demonstrated no contrast extravasation, and she was advanced to a full liquid diet. She was discharged home on post-operative day 7. A summary of the case can be seen in Table 1.

Discussion
Diagnosis: Gallstone ileus is a rare complication of cholelithiasis that necessitates urgent surgical intervention. Due to its nonspecific clinical presentation, initial diagnostic imaging typically includes an abdominal X-ray, which may reveal an ectopic gallstone in 33.33% of cases [4]. Additional findings can include dilated loops of small bowel or stomach and pneumobilia. However, given its limited sensitivity, most patients subsequently undergo computed tomography (CT), which has a reported sensitivity of 93% and can frequently identify an associated bilioenteric fistula [5].
Management: Surgical management of gallstone ileus has 3 main areas of consideration: relief of obstruction, management of cholelithiasis, and management of the underlying bilioenteric fistula. The primary concern is to relieve the obstruction. Small stones may be removed through minimally invasive techniques, including endoscopically with a basket device. Larger stones may be treated endoscopically as well, but may require advanced techniques including electrohydraulic lithotripsy or laser lithotripsy for easier removal. These techniques have a relatively low success rate, as low as 29% for Bouveret syndrome and decreasing success for more distal obstructions, and have an increased risk of complications including stone migration, bowel injury, and perforation [6]. In the presented case, the patient had a closed-loop small bowel obstruction as well as a gastric outlet obstruction requiring surgical intervention, as endoscopic removal of the proximal stone would not resolve any distal obstruction.
Surgical Decisions: Surgical management may be performed open or laparoscopically, and the approach depends on patient and surgeon factors. In both approaches, it is necessary to perform thorough inspection of the bowel to identify additional ectopic gallstones that could lead to obstruction [7]. Similar to Bouveret syndrome, gallstone ileus management is guided by surgeon experience and preference, with the bowel inspected for the point of obstruction. Stone extraction is achieved via a longitudinal enterotomy or, if bowel integrity is compromised, via segmental resection.
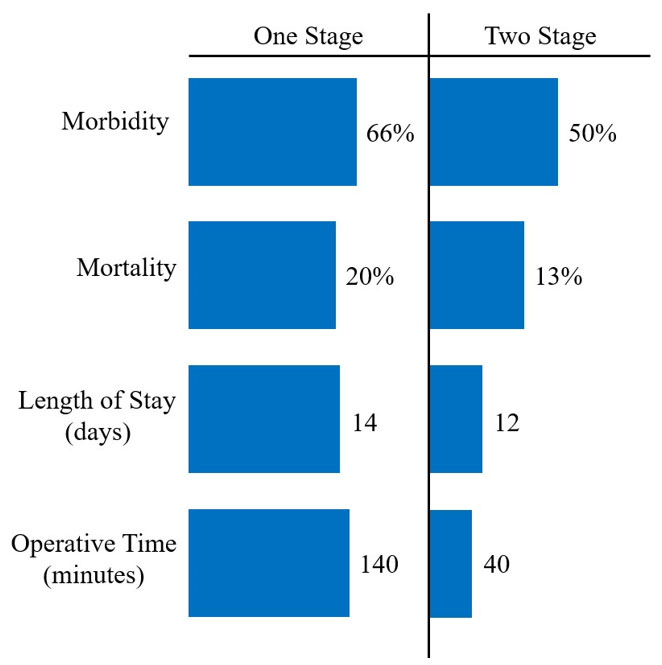
The choice to perform cholecystoenteric fistula take-down at the index operation remains controversial. Spontaneous closure of the fistula occurs in approximately 61.5% of cases, however, if left untreated, there is a risk of recurrence, up to 60% risk of cholangitis, and 15% chance of gallbladder cancer [8]. However, several studies have shown an increase in morbidity, mortality, length of stay, and operative times in patients who undergo a one-stage procedure (Figure 3) [9],[10],[11]. Performing a cholecystectomy with fistula closure is technically complex, and surgeons need to consider patient stability, ability to tolerate a prolonged procedure, risk of complications, and likelihood of healing spontaneously.
Conclusion
In this case of Twin-Stone syndrome, the closed-loop bowel obstruction and concomitant gastric outlet obstruction from dual stone impaction, and the presence of a cholecystoenteric fistula required urgent surgical intervention and reconstruction during the index operation. This case highlights both diagnostic and therapeutic challenges associated with Twin-Stone syndrome and the importance of patient-specific treatment.
REFERENCES
1.
Halabi WJ, Kang CY, Ketana N, Lafaro KJ, Nguyen VQ, Stamos MJ, et al. Surgery for gallstone ileus: A nationwide comparison of trends and outcomes. Ann Surg 2014;259(2):329–35. [CrossRef]
[Pubmed]

2.
Turner AR, Sharma B, Mukherjee S. Gallstone ileus. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
[Pubmed]
3.
Haddad FG, Mansour W, Deeb L. Bouveret’s syndrome: Literature review. Cureus 2018;10(3):e2299. [CrossRef]
[Pubmed]
4.
Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, Mazzeo R. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol 2004;50(1):23–9. [CrossRef]
[Pubmed]
5.
García-Quijada García J, Valle Rubio A, Pastor Riquelme P, Serantes Gómez A. Case report: Closed-loop bowel obstruction secondary to a double gallstone ileus. Int J Surg Case Rep 2021;89:106612. [CrossRef]
[Pubmed]
6.
Ong J, Swift C, Stokell BG, Ong S, Lucarelli P, Shankar A, et al. Bouveret syndrome: A systematic review of endoscopic therapy and a novel predictive tool to aid in management. J Clin Gastroenterol 2020;54(9):758–68. [CrossRef]
[Pubmed]
7.
Caldwell KM, Lee SJ, Leggett PL, Bajwa KS, Mehta SS, Shah SK. Bouveret syndrome: Current management strategies. Clin Exp Gastroenterol 2018;11:69–75. [CrossRef]
[Pubmed]
8.
Inukai K. Gallstone ileus: A review. BMJ Open Gastroenterol 2019;6(1):e000344. [CrossRef]
[Pubmed]
9.
Dai XZ, Li GQ, Zhang F, Wang XH, Zhang CY. Gallstone ileus: Case report and literature review. World J Gastroenterol 2013;19(33):5586–9. [CrossRef]
[Pubmed]
10.
Ravikumar R, Williams JG. The operative management of gallstone ileus. Ann R Coll Surg Engl 2010;92(4):279–81. [CrossRef]
[Pubmed]
11.
Doko M, Zovak M, Kopljar M, Glavan E, Ljubicic N, Hochstädter H. Comparison of surgical treatments of gallstone ileus: Preliminary report. World J Surg 2003;27(4):400–4. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
T N Hess - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Olivia N Brigando - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Daniel W Bailey - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 T N Hess et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}