 |
Case Report
The use of polymethyl methacrylate as an effective tamponade for a vertebral artery injury during anterior cervical corpectomy and fusion: A case report
1 Medical Student, College of Medicine, Howard University, Washington, DC, USA
2 Chief of Neurosurgery, Neurosurgical Department, Howard University Hospital, Washington, DC, USA
Address correspondence to:
Christopher McGinley
8200 Dixon Ave, Apt. 1002, Silver Spring, Maryland 20910,
USA
Message to Corresponding Author
Article ID: 100161Z12CM2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
McGinley C, Fossett D. The use of polymethyl methacrylate as an effective tamponade for a vertebral artery injury during anterior cervical corpectomy and fusion: A case report. J Case Rep Images Surg 2025;11(2):14–18.ABSTRACT
Introduction: Injury to the vertebral artery (VA) during an anterior cervical approach to the spine is relatively uncommon. These injuries can be difficult to repair, may lead to significant complications, and can even be fatal. We present a case report involving a VA injury that occurred during an anterior cervical corpectomy and fusion and discuss its management.
Case Report: A 65-year-old man presented with a chief complaint of radicular left upper extremity pain without weakness, numbness, or paresthesia. Imaging revealed cervical spondylosis with a kyphotic deformity. An anterior cervical corpectomy and fusion was recommended and the patient agreed to proceed with the surgery. During the drilling of the vertebral body, the left lateral wall of the vertebral body was inadvertently perforated, resulting in an injury to the VA. To address this complication polymethyl methacrylate (PMMA) was placed in the defect to replace the vertebral body and provide effective tamponade against the bleed.
Conclusion: Polymethylmethacrylate can be a very effective tool to use in the management of an injury to the VA, providing the ability to tamponade while simultaneously helping to maintain structural integrity and spinal stability.
Keywords: Cervical spine, Polymethyl methacrylate, Vertebral artery
Introduction
Anterior cervical corpectomy and fusion (ACCF) via the Smith–Robinson approach is commonly used by spine surgeons to manage compression of the anterior spinal cord [1],[2],[3],[4],[5] [6],[7]. The intervertebral discs above and below the affected vertebral segment(s) are removed, and the interstices of the vertebral body are drilled away, leaving only a protective shell of bone on each side. The resulting defect is then filled with a graft or prosthesis to maintain structural integrity and spinal stability. Depending on the material used to replace the vertebral body, an anterior cervical plate may be attached to the bone above and below to support the fusion and prevent migration of the prosthesis.
Injuries to the vertebral artery (VA) can be a serious complication of cervical spine surgery and are most likely to occur in three areas: (1) anteriorly at the C7 vertebra, (2) laterally between C3 and C7, and (3) posteriorly at C1 and C2 levels [8]. Vertebral arterial injuries tend to occur more frequently during posterior cervical approaches (4.1–8.2%) than they do with anterior cervical approaches (0.3–0.5%) [7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18].
To our knowledge, there is only one previously documented instance of using PMMA for vascular tamponade. In that case, a 73-year-old female experienced an unintended needle advancement during a transpedicular vertebroplasty, resulting in a thoracic aortic artery dissection [17]. Thanks to the surgeon’s quick thinking, PMMA was used as a tamponade for the bleeding. The intervention successfully stopped the bleeding, and the patient did not experience any untoward complications. We present a case involving the use of PMMA in a patient who suffered an iatrogenic injury to the left vertebral artery during an anterior cervical corpectomy and fusion procedure. The surgeon’s rapid response allowed the PMMA to effectively tamponade the bleeding, resulting in no adverse consequences.
Case Report
A 65-year-old man presented with left arm pain, which he rated a 10/10 on the visual analog scale (VAS). The pain involved the left shoulder, upper arm, forearm, and hand and was described as a constant, aching pain that began gradually, worsened with overhead activity and lifting, and was relieved by rest. The patient did not report any neck pain, lower extremity pain, weakness, numbness, tingling, or paresthesias. His symptoms were not significantly relieved with non-steroidal anti-inflammatory medications and muscle relaxants. He had undergone one course of physical therapy prior to his initial office visit, but it did not help relieve his symptoms.
On physical exam, the patient showed no evidence of weakness, numbness, paresthesias, or abnormal reflexes. Neither the Spurling’s test nor axial loading caused any discomfort. His past medical history was significant for hypertension, diabetes, hypercholesterolemia, gastrointestinal reflux disorder, benign prostatic hyperplasia, and a seizure disorder. All of his medical conditions were well controlled with medication.
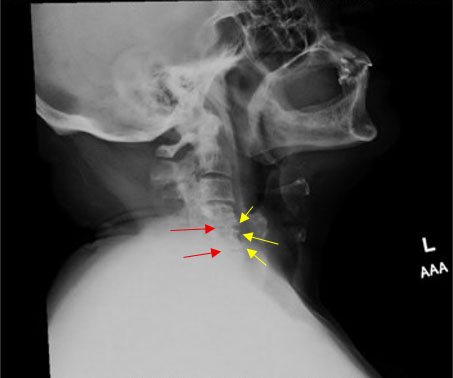
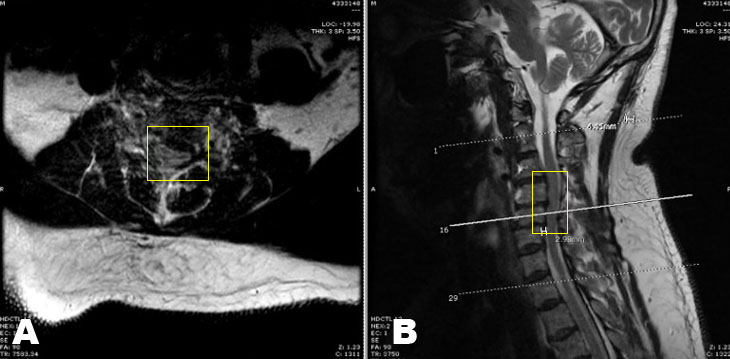
Plain X-ray imaging completed before his initial consultation revealed significant cervical spondylotic disease. There was loss of the normal cervical lordosis and marked narrowing of the intervertebral disc spaces, with degenerative changes identified most significantly at C4-5 and C5-6. The intervertebral disc spaces below the level of C5-6 were suboptimally visualized. Mild narrowing of the C5-6 neuroforamen on the left was noted (Figure 1). He was given a referral for another course of physical therapy, placed on a non-steroidal anti-inflammatory agent (NSAID) and a muscle relaxer, and sent for a magnetic resonance imaging study (MRI). The MRI validated the plain film imaging in that it revealed a C4-C5 and C5-C6 spondylosis, a mild posterior subluxation of C5 on C6, and a resultant kyphotic deformity. There was mild spinal canal narrowing at C4-C5 and C5-C6 without evidence of cord edema (Figure 2A and Figure 2B). The patient did not experience any symptomatic relief despite undergoing medicinal management and physical therapy; therefore, given the spondylotic changes seen on imaging, a recommendation was made for an anterior cervical corpectomy at C4 and C5 with fusion.
During the procedure, there were instances of excessive bone bleeding while drilling into the vertebral body despite the patient having no known bleeding disorders. Mid-procedure, the lateral wall of the vertebral body was accidentally perforated by the drill, resulting in significant arterial bleeding and indicating an injury to the vertebral artery. The anesthesiologist was alerted to this unfortunate occurrence, and hemostasis in the surgical field was temporarily achieved using gelfoam, thrombin, and digital pressure. Cardiovascular stability was maintained throughout the procedure.
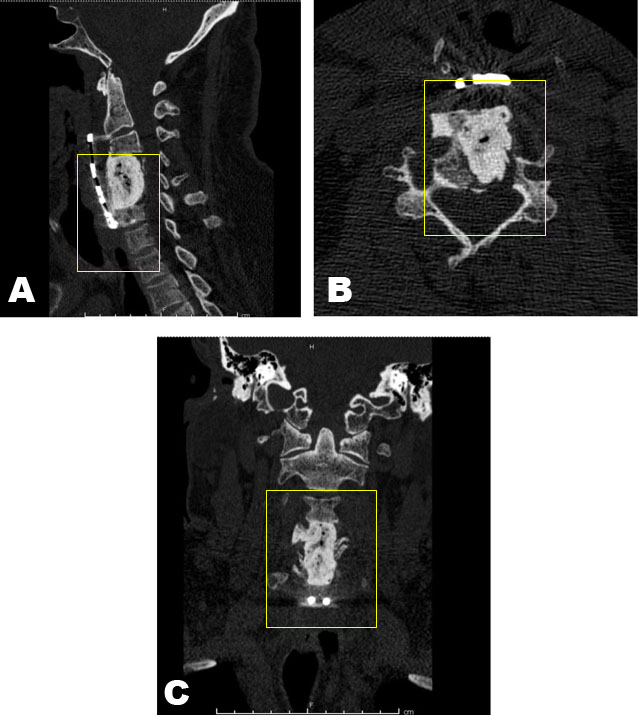
Polymethyl methacrylate (PMMA) was then prepared, and while still malleable but nearly rigid, digital pressure was released, and the PMMA was placed into the defect, where it quickly completed the hardening process in situ. All bleeding ceased immediately. Vital signs remained stable, and there were no changes in electrophysiological monitoring during the case. An anterior cervical plate was hastily affixed, the surgical wound was closed, and the patient was awakened, extubated, and found to be neurologically intact (Figure 3A, Figure 3B, Figure 3C). He was subsequently sent to a local institution for digital angiography to assess the vertebral artery. The angiogram showed complete occlusion of the vertebral artery at the level of injury, with back-filing of the distal vertebral artery from the Basilar artery.
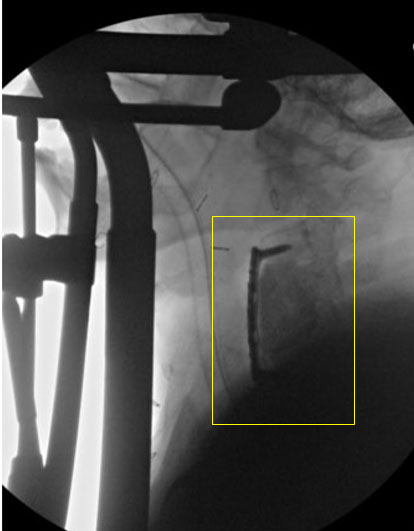
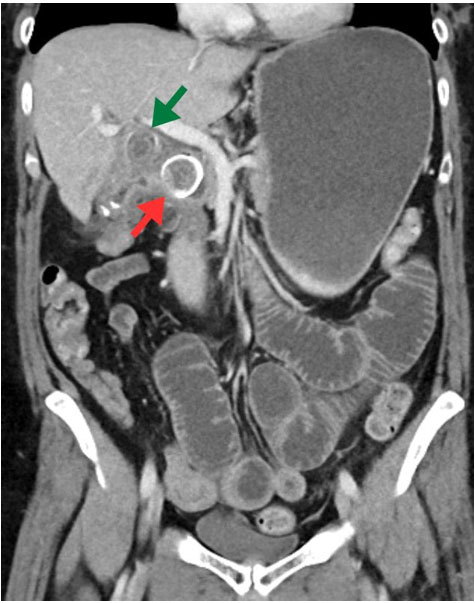
When he presented for his one-month follow-up, the patient’s only complaints were some difficulty swallowing larger bites of food and minimal paresthesias in both palms. The rest of his examination was unremarkable. Computed tomography (CT) imaging done to evaluate his swallowing difficulty disclosed that his hastily placed anterior cervical plate was poorly positioned. He underwent an uncomplicated revision surgery to adjust the cervical plate, and this correction completely resolved his swallowing difficulties (Figure 4).
Discussion
Although vertebral artery (VA) injuries are rare, they can result in serious complications such as lacerations, fistulas, pseudoaneurysms, and dissections. These injuries may result in cerebral ischemia, cranial nerve deficits, or even death. Therefore, it is crucial for surgeons to have not only a thorough understanding of the three-dimensional anatomy of the VA and its relationship to the cervical spine but also detailed knowledge of instrumentation techniques used in both anterior and posterior cervical spine surgeries.
There are no foolproof ways to prevent VA injuries in anterior cervical spine surgery, and aside from neuronavigation techniques, there are few, if any, definitive methods to prevent such injuries from occurring in posterior cervical spine surgery. There is, however, a consensus on how to manage such injuries should they occur. The primary goals are (1) controlling local hemorrhage, (2) preventing immediate vertebrobasilar ischemia, and (3) avoiding cerebral embolic complications. The anesthesiologist should be made aware of the issue and maintain constant communication with the surgeon regarding the need for fluid resuscitation or medications to augment blood pressure. These physiologic interventions help maintain cerebral perfusion pressure and can reduce the risk of ischemia in territories supplied by the posterior circulation.
Polymethyl methacrylate (PMMA) is a synthetic resin produced from the polymerization of methyl methacrylate. Commonly referred to as bone cement, PMMA should not be confused with bone wax, a combination of beeswax and a softening agent used to occlude porous venous channels in bone [19]. Polymethyl methacrylate was first produced in the 1930s by Hill and Crawford [19],[20],[21],[22]. Originally, it was not intended for medical use; however, in 1937, it was introduced to the dental field for use in powder form to fabricate dentures [23].
In the mid-1950s, PMMA was introduced to the surgical world through the work of orthopedic surgeons Saha and Pal [24]. Today, it remains one of the most widely used materials in Orthopedic surgery. Its transparency, biocompatibility, reliability, relative ease of manipulation, and low toxicity were soon seized upon and incorporated by many different medical specialties. Polymethyl methacrylate has been used for (a) bone cement; (b) contact and intraocular lens; (c) screw fixation in bone; (d) filler for bone cavities and skull defects; and (e) vertebrae stabilization in osteoporotic patients [22]. Although numerous new alloplastic materials show promise, the versatility and reliability of PMMA make it remain a popular and frequently used material [22].
Currently, there are three surgical options for the management of an intraoperative VA injury: (1) hemostatic tamponade, (2) microvascular repair of the injured artery, and (3) ligation or occlusion of the artery either directly or via an endovascular approach. Gelfoam (Pfizer, USA), Surgicel (Johnson & Johnson, USA), or bone wax are frequently used as hemostatic agents in spine surgery and are often effective in controlling bleeding. However, there have been several reported cases of delayed hemorrhage and fistula formation resulting from packing the injured artery [25],[26],[27]. Microvascular repair aims to restore normal blood flow in order to diminish the risk of immediate or delayed ischemic complications, but it is technically challenging, particularly in the setting of anterior spinal surgery [9],[17],[25],[27]. Ligation of the VA carries significant risks, including cerebellar or brain stem infarction and isolated cranial nerve paresis, with a reported mortality of 12% [25],[28],[29]. If direct vessel repair is not possible and ligation is necessary, intraoperative angiography should be considered. It should be noted that the vessel must be ligated both proximally and distally. If only proximal ligation is performed, there is a risk of causing delayed embolic or hemorrhagic events, and fistula formation can occur [9],[26],[27]. There is no one preferred strategy for managing intraoperative hemorrhagic issues with the vertebral artery.
Conclusion
Management of VA injuries in cervical spine surgery is not homogenous. Each event requires a tailored management strategy to optimize outcomes. The use of PMMA to tamponade the artery proved to be an effective strategy in our case. Concomitantly, PMMA provided structural stability and helped maintain overall spinal integrity. Surgeons should be prepared for potential complications during their procedures and have management options available for intra-operative mishaps. The versatility of PMMA in certain situations can be a valuable tool to have in the spine surgeon’s toolkit.
REFERENCES
1.
Wen Z, Lu T, Wang Y, Liang H, Gao Z, He X. Anterior cervical corpectomy and fusion and anterior cervical discectomy and fusion using titanium mesh cages for treatment of degenerative cervical pathologies: A literature review. Med Sci Monit 2018;24:6398–404. [CrossRef]
[Pubmed]

2.
Jain V, Madan A, Thakur M, Thakur A. Functional outcomes of subaxial spine injuries managed with 2-level anterior cervical corpectomy and fusion: A prospective study. Neurospine 2018;15(4):368–75. [CrossRef]
[Pubmed]
3.
Hartmann S, Tschugg A, Obernauer J, Neururer S, Petr O, Thomé C. Cervical corpectomies: Results of a survey and review of the literature on diagnosis, indications, and surgical technique. Acta Neurochir (Wien) 2016;158(10):1859–67. [CrossRef]
[Pubmed]
4.
Theologis AA, Lansdown D, McClellan RT, Chou D, Pekmezci M. Multilevel corpectomy with anterior column reconstruction and plating for subaxial cervical osteomyelitis. Spine (Phila Pa 1976) 2016;41(18):E1088–95. [CrossRef]
[Pubmed]
5.
Wei-bing X, Wun-Jer S, Gang L, Yue Z, Ming-xi J, Lian-shun J. Reconstructive techniques study after anterior decompression of multilevel cervical spondylotic myelopathy. J Spinal Disord Tech 2009;22(7):511–5. [CrossRef]
[Pubmed]
6.
Shamji MF, Massicotte EM, Traynelis VC, Norvell DC, Hermsmeyer JT, Fehlings MG. Comparison of anterior surgical options for the treatment of multilevel cervical spondylotic myelopathy: A systematic review. Spine (Phila Pa 1976) 2013;38(22 Suppl 1):S195–209. [CrossRef]
[Pubmed]
7.
Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40-A(3):607–24.
[Pubmed]
8.
Abumi K, Shono Y, Ito M, Taneichi H, Kotani Y, Kaneda K. Complications of pedicle screw fixation in reconstructive surgery of the cervical spine. Spine (Phila Pa 1976) 2000;25(8):962–9. [CrossRef]
[Pubmed]
9.
Golfinos JG, Dickman CA, Zabramski JM, Sonntag VK, Spetzler RF. Repair of vertebral artery injury during anterior cervical decompression. Spine (Phila Pa 1976) 1994;19(22):2552–6. [CrossRef]
[Pubmed]
10.
Peng CW, Chou BT, Bendo JA, Spivak JM. Vertebral artery injury in cervical spine surgery: Anatomical considerations, management, and preventive measures. Spine J 2009;9(1):70–6. [CrossRef]
[Pubmed]
11.
Wright NM, Lauryssen C. Vertebral artery injury in C1-2 transarticular screw fixation: Results of a survey of the AANS/CNS section on disorders of the spine and peripheral nerves. American Association of Neurological Surgeons/Congress of Neurological Surgeons. J Neurosurg 1998;88(4):634–40. [CrossRef]
[Pubmed]
12.
Haid RW Jr, Subach BR, McLaughlin MR, Rodts GE Jr, Wahlig JB Jr. C1-C2 transarticular screw fixation for atlantoaxial instability: A 6-year experience. Neurosurgery 2001;49(1):65–8; discussion 69–70. [CrossRef]
[Pubmed]
13.
Madawi AA, Casey AT, Solanki GA, Tuite G, Veres R, Crockard HA. Radiological and anatomical evaluation of the atlantoaxial transarticular screw fixation technique. J Neurosurg 1997;86(6):961–8. [CrossRef]
[Pubmed]
14.
Deen HG, Birch BD, Wharen RE, Reimer R. Lateral mass screw-rod fixation of the cervical spine: A prospective clinical series with 1-year follow-up. Spine J 2003;3(6):489–95.
[Pubmed]
15.
Heller JG, Silcox DH 3rd, Sutterlin CE 3rd. Complications of posterior cervical plating. Spine (Phila Pa 1976) 1995;20(22):2442–8. [CrossRef]
[Pubmed]
16.
Pateder DB, Carbone JJ. Lateral mass screw fixation for cervical spine trauma: Associated complications and efficacy in maintaining alignment. Spine J 2006;6(1):40–3. [CrossRef]
[Pubmed]
17.
Daentzer D, Deinsberger W, Böker DK. Vertebral artery complications in anterior approaches to the cervical spine: Report of two cases and review of literature. Surg Neurol 2003;59(4):300–9. [CrossRef]
[Pubmed]
18.
Burke JP, Gerszten PC, Welch WC. Iatrogenic vertebral artery injury during anterior cervical spine surgery. Spine J 2005;5(5):508–14. [CrossRef]
[Pubmed]
19.
Zhou H, Ge J, Bai Y, Liang C, Yang L. Translation of bone wax and its substitutes: History, clinical status and future directions. J Orthop Translat 2019;17:64–72. [CrossRef]
[Pubmed]
20.
Raszewski Z, Nowakowska-Toporowska A, Nowakowska D, Więckiewicz W. Update on acrylic resins used in dentistry. Mini Rev Med Chem 2021;21(15):2130–7. [CrossRef]
[Pubmed]
21.
Kostić M, Igić M, Gligorijević N, Nikolić V, Stošić N, Nikolić L. The use of acrylate polymers in dentistry. Polymers (Basel) 2022;14(21):4511. [CrossRef]
[Pubmed]
22.
Frazer RQ, Byron RT, Osborne PB, West KP. PMMA: An essential material in medicine and dentistry. J Long Term Eff Med Implants 2005;15(6):629–39. [CrossRef]
[Pubmed]
23.
Peyton FA. History of resins in dentistry. Dent Clin North Am 1975;19(2):211–22.
[Pubmed]
24.
Saha S, Pal S. Mechanical properties of bone cement: A review. J Biomed Mater Res 1984;18(4):435–62. [CrossRef]
[Pubmed]
25.
Smith MD, Emery SE, Dudley A, Murray KJ, Leventhal M. Vertebral artery injury during anterior decompression of the cervical spine. A retrospective review of ten patients. J Bone Joint Surg Br 1993;75(3):410–5. [CrossRef]
[Pubmed]
26.
Cosgrove GR, Théron J. Vertebral arteriovenous fistula following anterior cervical spine surgery. Report of two cases. J Neurosurg 1987;66(2):297–9. [CrossRef]
[Pubmed]
27.
de los Reyes RA, Moser FG, Sachs DP, Boehm FH. Direct repair of an extracranial vertebral artery pseudoaneurysm: Case report and review of the literature. Neurosurgery 1990;26(3):528–33. [CrossRef]
[Pubmed]
28.
Shintani A, Zervas NT. Consequence of ligation of the vertebral artery. J Neurosurg 1972;36(4):447–50. [CrossRef]
[Pubmed]
29.
Golueke P, Sclafani S, Phillips T, Goldstein A, Scalea T, Duncan A. Vertebral artery injury—diagnosis and management. J Trauma 1987;27(8):856–65.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Christopher McGinley - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Damirez Fossett - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Christopher McGinley et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}