 |
Case Report
Intracholecystic papillary neoplasm in a child: A case report
1 Loma Linda University School of Medicine, Loma Linda, CA, USA
2 Department of Surgery, Division of Pediatric Surgery, Loma Linda University Health, Loma Linda, CA, USA
3 Department of Pathology and Human Anatomy, Loma Linda University School of Medicine, Loma Linda, CA, USA
Address correspondence to:
Vinicius Silva
24920 Mound St., Loma Linda, CA 92350,
USA
Message to Corresponding Author
Article ID: 100163Z12VS2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Silva V, McRae J, Deisch J, Mladenov G, Kashtan M, Mejaddam A. Intracholecystic papillary neoplasm in a child: A case report. J Case Rep Images Surg 2025;11(2):24–28.ABSTRACT
Introduction: Gallbladder (GB) cancer is a well-studied neoplasia that occurs within the mucosal lining of the gallbladder. More recently, a pre-invasive lesion of the gallbladder, known as intracholecystic papillary neoplasm (ICPN), has been described in the literature. Intracholecystic papillary neoplasm is rare in the adult population and is commonly found incidentally after cholecystectomy. In pediatric care, only one such case has previously been documented.
Case Report: Our patient, an 11-year-old male with a history of immunosuppressant use for nephrotic syndrome, presented with symptoms suspicious for choledocholithiasis. He was found to have ICPN on histopathological analysis after cholecystectomy. Post-operative course was notable for biliary obstruction due to hemobilia that required endoscopic retrograde cholangiopancreatography (ERCP) with stent placement.
Conclusion: Cholecystectomy and scheduled follow-up are a suitable way of preventing the progression of ICPN. Pediatric patients should also be considered for genetic testing.
Keywords: Choledocholithiasis, Immunosuppression, Intracholecystic papillary neoplasm, Pediatric
Introduction
Intracholecystic papillary neoplasm (ICPN) is a rare pre-malignant neoplasm of the gallbladder (GB), most often diagnosed incidentally after cholecystectomy. Originally described in the adult population in 2012, it is defined as an exophytic GB mass =1.0 cm in size composed of pre-invasive cells that are distinct from the neighboring mucosa [1]. The size requirement differentiates it from other types of GB neoplasms, which tend to have flatter growth patterns [1]. Though ICPN itself is not malignant, it follows the adenoma-carcinoma sequence [1],[2],[3],[4], with more than half of adult cases being associated with invasive cancer [1],[2],[4]. Outcomes between studies vary on whether ICPN-associated cancer has a similar or better prognosis than conventional GB cancer after T-stage matching [1],[5]. Therefore, although the prevalence of ICPN is low [2], it still warrants concern for malignancy if detected. Pediatric cases of ICPN are extremely rare, having been documented only once before [6]. Here, we present the second known pediatric case of ICPN.
Case Report
The patient, an 11-year-old male, presented to the Emergency Department with a 2-day history of fatigue that progressed to abdominal pain and more than 10 episodes of non-bloody emesis on the day before presentation. His past medical history was significant for steroid-resistant nephrotic syndrome secondary to membranous nephropathy (MN) and focal segmental glomerulosclerosis (FSGS), diagnosed by histopathology seven months prior and controlled with tacrolimus. However, the patient could not obtain tacrolimus for two weeks before his presentation. He denied diarrhea, constipation, hematochezia, or melena. The patient’s temperature and heart rate were within normal limits, but he was tachypneic and hypertensive (149/106 mmHg).
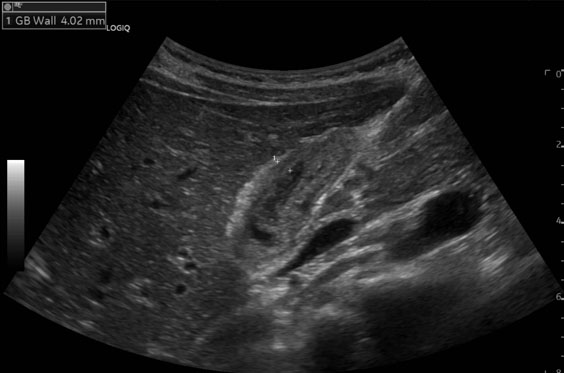
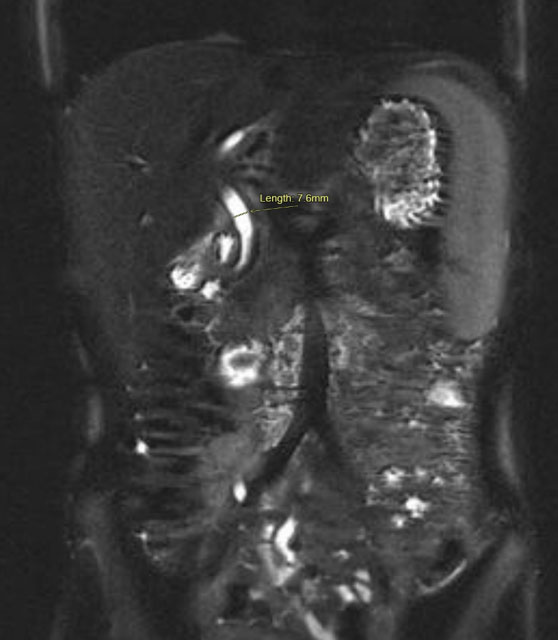
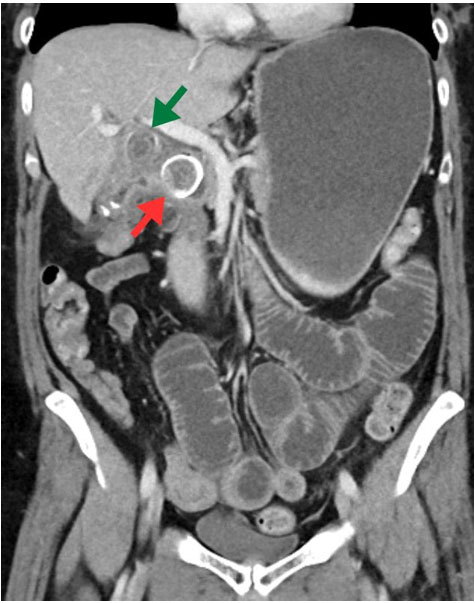
On physical exam, the patient had epigastric tenderness. Preoperative labs were notable for leukocytosis, hypoalbuminemia, direct hyperbilirubinemia (direct bilirubin of 2.8 mg/dL, total bilirubin of 2.9 mg/dL), elevated alkaline phosphatase, elevated aspartate aminotransferase, elevated alanine aminotransferase, and mildly elevated lipase. An abdominal ultrasound showed a thickened GB wall and a dilated common bile duct (CBD) (Figure 1). Due to suspicion of biliary tract disease, he underwent magnetic resonance cholangiopancreatography (MRCP), which showed a CBD diameter of 7.6 mm without evidence of choledocholithiasis or definitive evidence of cholecystitis (Figure 2). Because of concerns for a passed gallstone, he underwent inpatient laparoscopic cholecystectomy three days later.
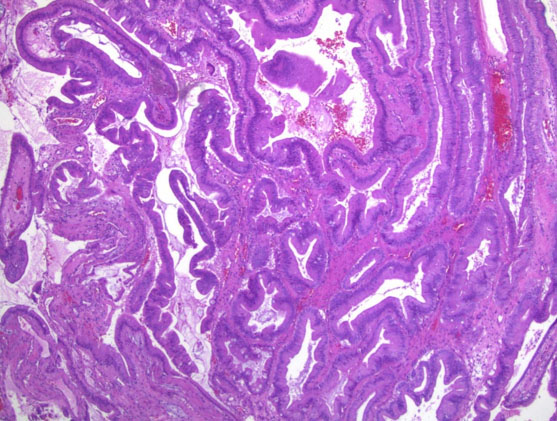
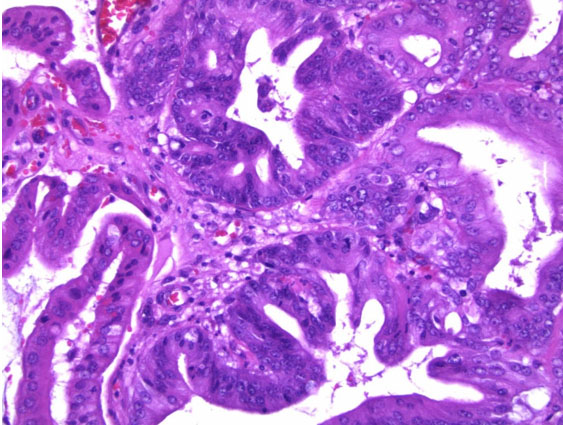
The GB was submitted to pathology for examination. Gross inspection demonstrated an intact saccular GB measuring 5.5 × 2 × 1.5 cm, without mural perforation. The GB lumen contained viscous green bile; no obstruction of the cystic duct or intraluminal calculi were seen. The GB wall was thin, without hemorrhage, significant inflammation, or edema. There was a 1.5 cm soft tan exophytic mucosal mass present within the body of the GB. Histological sections taken from the GB wall, cystic duct margin, and the mass demonstrated a complex adenomatous epithelial proliferation with a tubulopapillary growth pattern and intestinal-type differentiation. There was patchy accentuated cytologic atypia and glandular irregularity, consistent with high-grade dysplasia (Figure 3 and Figure 4). There was no evidence of stromal infiltration present to suggest invasive malignancy. The cystic duct margin was uninvolved by dysplasia. Based upon these findings, a diagnosis of ICPN with high-grade dysplasia was reported.
On postoperative day 1, the patient’s total bilirubin and direct bilirubin rose to 2.4 and 0.9 mg/dL, respectively, which prompted another MRCP. This MRCP showed significant CBD dilation with filling defects and occlusion of the distal end of the CBD. Endoscopic retrograde cholangiopancreatography (ERCP) was performed the following day, which showed blood in the duodenum and a large clot protruding from the distal CBD through the ampulla. The blood was suctioned, the clot was removed, and a stent was placed for residual drainage. The patient was discharged two days later for a total postoperative stay of four days.
At a follow-up visit in the clinic, the patient was doing well without signs of abdominal pain. A scheduled follow-up ERCP three months later showed a dilated CBD and distal filling defects, this time with associated sludge and stone debris. The bile duct was swept with a balloon, the stent was removed, bile flow was restored, and the patient was discharged the same day.
The surveillance plan for the patient included a follow-up with genetic testing and clinical monitoring. However, the patient was lost to follow-up.
Discussion
Intracholecystic papillary neoplasm is rare and more common in adults than in pediatrics. Thus, most information is derived from adult literature. The most common presenting symptom is right upper quadrant pain, though half of all cases may be asymptomatic [1],[2]. Imaging [ultrasound, magnetic resonance imaging (MRI), and computed tomography (CT)] is the best non-invasive modality to assess for ICPN [3],[7].[8],[9]; however, a definitive diagnosis is made through histopathological evaluation [1]. Although risk factors for the development of ICPN specifically are yet unknown, there is a well-established link between immunosuppression and neoplasia. This is due in part to an impaired ability of the immune system to detect and eliminate carcinogenic antigens [10]. Our patient’s long-term history of immunosuppression may have contributed to his development of ICPN.
Because ICPN is slowly progressing, it tends to be diagnosed at earlier stages than conventional GB carcinoma. Thus, the outcomes of patients with ICPN tend to be more favorable than those who have conventional GB carcinoma, even if the ICPN is associated with invasive cancer (ICPN-C) [1],[5],[11],[12]. Cholecystectomy is therefore a suitable treatment option for a diagnosis of ICPN.
The only other case of ICPN reported was a previously healthy 15-year-old female with a 6-month history of abdominal pain who was discovered to have choledocholithiasis by ultrasound [6]. She underwent cholecystectomy, and the discovery of ICPN was made during pathological evaluation. Because of the patient’s age, genetic testing was ordered to evaluate the risk of other malignancies. Though the testing did not show significant results in that case, clinicians may still consider recommending genetic testing for pediatric patients diagnosed with ICPN to screen for concurrent disease potential.
Conclusion
Intracholecystic papillary neoplasm is a rare pre-cancerous lesion of the gallbladder that may be associated with invasive carcinoma. The diagnosis is confirmed upon histopathologic evaluation of a resected gallbladder. This lesion is rare in the pediatric population, where only one case has previously been documented. Intracholecystic papillary neoplasm and ICPN-C generally have better outcomes than conventional gallbladder cancer (GBC), but similar management methods should be considered for both, especially in cases of high grade ICPN-C. Additionally, pediatric patients may benefit from genetic testing to screen for concurrent predispositions.
REFERENCES
1.
Adsay V, Jang KT, Roa JC, Dursun N, Ohike N, Bagci P, et al. Intracholecystic papillary-tubular neoplasms (ICPN) of the gallbladder (neoplastic polyps, adenomas, and papillary neoplasms that are ≥1.0 cm): Clinicopathologic and immunohistochemical analysis of 123 cases. Am J Surg Pathol 2012;36(9):1279–301. [CrossRef]
[Pubmed]

2.
Kiruthiga KG, Kodiatte TA, Burad D, Kurian R, Raju RS, Rymbai ML, et al. Intracholecystic papillary-tubular neoplasms of the gallbladder – A clinicopathological study of 36 cases. Ann Diagn Pathol 2019;40:88–93. [CrossRef]
[Pubmed]
3.
Arfan S, Sharma K, Anbazhagan L, Stear TJ. A rare finding of incidental intracholecystic papillary neoplasm following acute cholecystitis management. Cureus 2023;15(6):e41222. [CrossRef]
[Pubmed]
4.
Bennett S, Marginean EC, Paquin-Gobeil M, Wasserman J, Weaver J, Mimeault R, et al. Clinical and pathological features of intraductal papillary neoplasm of the biliary tract and gallbladder. HPB (Oxford) 2015;17(9):811–8. [CrossRef]
[Pubmed]
5.
Kang JS, Lee KB, Choi YJ, Byun Y, Han Y, Kim H, et al. A comparison of outcomes in patients with intracholecystic papillary neoplasms or conventional adenocarcinomas of the gallbladder. HPB (Oxford) 2021;23(5):746–52. [CrossRef]
[Pubmed]
6.
McClellan JM, Escobar MA Jr. Intracholecystic papillary-tubular neoplasm of the gallbladder presenting. Journal of Pediatric Surgery Case Reports 2017;25:46–48. [CrossRef]
7.
Watanabe Y, Mochidome N, Nakayama H, Gotoh Y, Setoguchi T, Sunami S, et al. Intracholecystic papillary neoplasm associated with invasive carcinoma of the remnant gallbladder after subtotal cholecystectomy: A case report. Surg Case Rep 2022;8(1):31. [CrossRef]
[Pubmed]
8.
Koike D, Kato H, Asano Y, Ito M, Arakawa S, Kawabe N, et al. Natural history of intracholecystic papillary neoplasm (ICPN): A rare case of ICPN whose natural history was closely followed by ultrasound. BMC Gastroenterol 2022;22(1):377. [CrossRef]
[Pubmed]
9.
Fujii Y, Noda Y, Koshita S, Kanno Y, Ogawa T, Kusunose H, et al. Intracholecystic papillary-tubular neoplasm of the gallbladder originating in the cystic duct with extensive intraepithelial progress in the common bile duct. Clin J Gastroenterol 2019;12(3):197–204. [CrossRef]
[Pubmed]
10.
Vial T, Descotes J. Immunosuppressive drugs and cancer. Toxicology 2003;185(3):229–40. [CrossRef]
[Pubmed]
11.
Akita M, Fujikura K, Ajiki T, Fukumoto T, Otani K, Hirose T, et al. Intracholecystic papillary neoplasms are distinct from papillary gallbladder cancers: A clinicopathologic and exome-sequencing study. Am J Surg Pathol 2019;43(6):783–91. [CrossRef]
[Pubmed]
12.
Berger Y, Sullivan BJ, Leigh NL, Bekhor EY, Dhorajiya P, Mani M, et al. Gallbladder cancer: A single-institution 10-year experience—Analysis of adenocarcinoma subtypes and tumors arising from intracholecystic papillary neoplasms. Ann Surg Oncol 2022;29(8):5167–75. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Vinicius Silva - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Joyce McRae - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jeremy Deisch - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Georgi Mladenov - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mark Kashtan - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ali Mejaddam - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AcknowledgmentsArtificial intelligence (AI) uses in the article: No artificial intelligence has been used in any part of the creation or revision of this manuscript.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Vinicius Silva et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}