 |
Case Report
Challenges in the management of a rare congenital extragonadal teratoma in a resource constrained setting: A case report
1 Department of Surgery, Ebonyi State University Abakaliki, Ebonyi State, Nigeria
2 Department of Surgery, Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Nigeria
3 Department of Surgery, University of Uyo Teaching Hospital, Uyo, Nigeria
Address correspondence to:
Akputa Aja Obasi
Ebonyi State University Abakaliki, Ebonyi State,
Nigeria
Message to Corresponding Author
Article ID: 100168Z12AO2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Obasi AA, Omebe WES, Akpaette IC. Challenges in the management of a rare congenital extragonadal teratoma in a resource constrained setting: A case report. J Case Rep Images Surg 2026;12(1):15–19.ABSTRACT
Introduction: Teratomas, which are the commonest germ cell tumors in children, could be gonadal or extragonadal in location. The head and neck region is a rare extragonadal site. A common site for head and neck teratomas is the cervical region. Congenital cervical teratomas can grow to huge proportions, posing significant airway and other management challenges. Although these challenges are universal, some are more pronounced in resource constrained settings.
Case Report: We present our experience with a 3-month-old infant who had a progressively increasing left anterolateral congenital neck mass which caused respiratory distress at two months of age. Intubation was achieved with the aid of a videolaryngoscope and the mass was successfully resected. The mass weighed 300 grams and measured 10 × 7.5 × 2.5 cm. Pathology showed tissue derivatives of the three germ cell layers and the histologic diagnosis was mature teratoma.
Conclusion: Lack of prenatal diagnosis, delayed postnatal diagnosis, absence of Multidisciplinary team management and non-compliance with recommended follow-up regimen are challenges of managing congenital cervical teratomas in resource constrained settings. Thorough periodic physical examinations and ultrasound scan of the neck are recommended for the follow-up of mature cervical teratoma patients in resource-constrained environments.
Keywords: Challenge, Extragonadal, Respiratory distress, Teratoma
Introduction
Teratomas are tumors composed of tissues derived from all three germ cell layers but these tissues are foreign to their anatomical site of origin [1],[2]. They constitute the commonest germ cell tumors in children [2]. They could be found at gonadal or extragonadal sites [3],[4]. Extragonadal teratomas are commonly found in the sacrococcygeal region and mediastinum and rarely at the head and neck region of the body [3],[4]. Head and neck teratomas make up 2–5% of all germ cell tumors and 6% of all teratomas [2],[5],[6]. A common site for head and neck teratoma is the cervical region [6]. Congenital cervical teratoma can grow to huge proportions and pose significant management challenges [5],[6],[7],[8]. Although these challenges are universal, some are more pronounced in resource-constrained settings. In this report, we share our experience in the successful management of an infant with a congenital cervical teratoma presenting in a resource-constrained setting, highlighting the management challenges and what lessons we learnt.
Case Report
A 3-month-old male infant who was delivered at term via a spontaneous vaginal delivery to a 27-year-old primiparous single woman was referred to our institution owing to a progressively increasing neck swelling noticed at birth. Four weeks prior to presentation, he had developed respiratory distress which worsened in the supine position but improved while lying prone. There was no difficulty in swallowing and no skin changes. Pregnancy had been largely unsupervised and no prenatal ultrasound scan (USS) was done.
Examination revealed a male infant with grunting respiration, chest indrawing, and subcostal recessions. A large oval-shaped midline cervical mass extending to the left was noted. It measured 10 × 9 × 9-cm with a bosselated appearance. The surface was irregular and it had no differential warmth. The mass had a mixed firm-soft consistency, and was mobile. It was not compressible, had no pulsation or bruit and the overlying skin was normal. Percussion over the manubrium was resonant (Figure 1). A diagnosis of congenital cervical teratoma was made.
A cervical US done at the onset of the respiratory distress, noted a huge, heterogenous mainly solid mass with multicystic spaces and multiple echogenic foci showing posterior acoustic shadowing suggestive of calcifications measuring 12 × 4.7 × 10-cm in the left anterolateral neck. The left carotid sheath was displaced posteriorly, the trachea to the contralateral side and the thyroid gland was separate from the mass. There was no significant blood flow on Doppler interrogation.
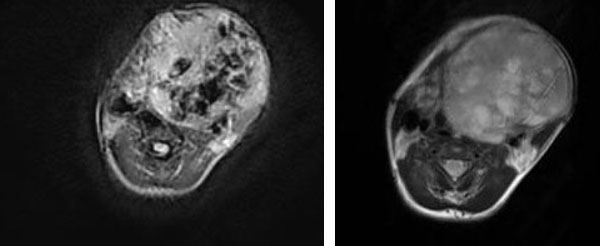
A magnetic resonance imaging (MRI) scan of the neck (Figure 2) showed a huge oval shaped, well marginated anterolateral neck mass, with lobulated outline, heterogenously hyperintense on T2-weighted images and hypointense on T1-weighted images. There were multiple irregular signal void areas representing calcifications. There was a mass effect from the mass on adjacent structures leading to tracheal and esophageal shift to the right, stretching of the strap muscles, the subcutaneous tissues and the skin. There was no evidence of adjacent tissue invasion.
Complete blood count and serum electrolytes, urea and creatinine (SEUC) were within normal reference range. Alpha fetoprotein (AFP) was not done owing to financial constraints.
He was optimized for surgery and an excision was done after planning with the anesthetist and ear, nose, and throat (ENT) surgeons. Following endotracheal intubation facilitated by video laryngoscopy, a left sided transverse skin crease incision was made over the swelling through the subcutaneous tissues, platysma and subplatysmal flaps raised. A grayish white well encapsulated mass underneath the thinned out and splayed infrahyoid strap muscles was mobilized by freeing its attachments to the muscles. Fibrous tissue strands and small blood vessels attaching it to the pretracheal fascia were transected to free it. The mass was neither attached to the thyroid gland nor the left carotid sheath.
There was no respiratory distress in the immediate postoperative period. He was however admitted into the intensive care unit (ICU) for observation, and was discharged home on postoperative day 6. He has remained well after three months of follow-up (Figure 3).
The resected mass weighed 300 g and measured 10 × 7.5 × 4.5 cm. It was composed of tissues derived from the ectodermal, mesodermal, and endodermal germ layers. No atypical cells were seen. The histologic diagnosis was mature teratoma.


Discussion
Head and neck teratomas which constitute 2–5% of all germ cell tumors are predominantly located in the neck [6]. With a propensity to grow to huge proportions, congenital cervical teratomas pose significant management challenges [5],[6],[7],[8]. Morbidity and mortality related to congenital cervical teratoma correlates with a high incidence of respiratory distress as a result of either tracheal compression or pulmonary hypoplasia [6],[7].[8]. The risk becomes more significant without perinatal diagnosis [6],[7].[8]. The risk of perinatal mortality, which was very high, has been reduced significantly with survival rates of 83% by prenatal diagnosis and ex utero intrapartum treatment (EXIT) procedure [7]. Although facilities are available for prenatal diagnosis, the mother of our patient had no prenatal ultrasound scan (USS) owing to financial constraints. She therefore ran the risk of fetal loss, birth dystocia, perinatal airway obstruction and perinatal mortality of her baby.
Prenatal diagnosis makes late presentation a rarity since in utero detection of a neck swelling guides prenatal counselling, antenatal care and post natal care [2]. Our patient presented after three months of delivery. The absence of respiratory distress at birth and inability to afford surgical care may have contributed to this. Delayed diagnosis due to lack of awareness that diagnosis and surgical intervention must be expedient in an infant with a congenital neck mass was evident too. Other factors responsible for late presentation in resource-constrained environments include initial refusal of surgery, prior inadequate excision by the unqualified and hidden tumor [9], and the misconception that infants cannot be safely operated.
The presence of a congenital neck mass in a neonate demands prompt and accurate diagnosis [10]. This is important in order to avoid delayed or inadequate treatment. Congenital neck masses could be cervical teratoma, hemangioma, congenital goiter, branchial cleft cysts, cervical neuroblastoma, lipoma, dermoid cyst, or laryngocele [10],[11]. Owing to the similarity in the location, patient’s age, sex and clinical presentation, it is paramount to differentiate a cervical teratoma from a cystic hygroma which is its closest differential [10]. Predominantly solid or mixed solid-cystic anterolateral congenital neck masses suggest cervical teratoma [8]. Cystic hygromas are soft in consistency and often located in the posterior triangle of the neck [12].
When a congenital anterolateral neck swelling is predominantly cystic, clinical differentiation of cervical teratoma from a cystic hygroma may be difficult [8],[10].
Imaging techniques like USS, computed tomography (CT) scan, and MRI are invaluable in distinguishing between these pathologies. Ultrasound scan of a teratoma shows a multiloculated, irregular, solid-cystic mass with calcifications [10]. In contrast, cystic hygromas appear as fluid-filled spaces of variable sizes separated by fine septae [10]. Where the diagnosis is in doubt following USS, CT scan, and MRI can clarify the diagnosis [10],[11].
In resource-poor settings, certain imaging challenges may be encountered. Firstly, inadequate radiologic investigative modalities or inexperienced operators giving equivocal results [9]. This in turn contributes to delay in diagnosis or treatment or inadequate treatment. Secondly, MRI with better tissue resolution and without radiation exposure is scarce and when available, expensive.
In our case, the radiological signs of a well circumscribed anterolateral cervical mass of heterogenous nature showing areas of calcifications on USS and MRI were suggestive of a teratoma thereby easily excluding a cystic hygroma.
With respect to diagnosing teratomas, AFP plays a limited and complimentary role to diagnostic imaging and histopathology [13],[14]. Alpha fetoprotein value at birth is variable and it is influenced by factors such as birth weight, gestational age, the presence of neural tube defects, anterior abdominal wall defects, certain germ cell tumors and hepatoblastoma [13],[14]. The AFP level generally decreases in infancy and so teratoma should be suspected when the AFP level remains high or increases in infancy [10],[13],[15]. Alpha fetoprotein plays a more definitive role in monitoring the effectiveness of surgical treatment [14]. Post-resection, the level of AFP is expected to fall [10]. However, persistence of high levels or increasing levels of AFP after resection are suggestive of incomplete resection, recurrence or malignant transformation [6],[11]. In this study, preoperative AFP could not be done owing to financial constraints. We therefore lost the opportunity to have a baseline for future comparisons. However previous research studies had suggested that AFP levels in infancy ought to be interpreted with caution and diagnostic imaging and histopathology should be prioritized over AFP [13],[14].
In the postpartum period, early and complete resection of a cervical teratoma should be the goal of treatment even in the absence of airway compromise [11]. Airway obstruction and airway management remains an ever present challenge in infants with cervical teratoma [2],[5]. Ex utero intrapartum treatment procedure to secure the airway cannot be done owing to non-existence of fetal Multidisciplinary team (MDT) at most centers in resource constrained settings [4]. The absence of pediatric anesthesiologist and fiber optic laryngoscopy in our setting makes post natal airway management daunting. Our patient was successfully intubated with the aid of a video laryngoscope. Otherwise airway management would require rigid bronchoscopy or tracheostomy. This becomes another challenge with the paucity of pediatric otolaryngologists and properly equipped neonatal intensive care unit (NICU) [9].
Long term follow up is recommended after resection. This will enhance prompt detection of inadequate excision, recurrence or malignant transformation. Use of Clinical examination, serial alpha fetoprotein (AFP) and MRI during follow-up visits are recommended [6]. Alpha fetoprotein should be obtained pre-excision, one month after excision, every three months for one year and then yearly for three years [11]. Magnetic resonance imaging is done biannually for the first three years [11]. Considering the high attrition rate of patients with neoplastic conditions in resource-constrained settings, this follow up guideline is impractical and would add additional financial burdens to parents of our patients who pay out of their pockets for health care [6],[16]. Thorough periodic physical examinations and ultrasound scan of the neck would be more practical and should be considered especially for mature teratoma patients [6].
Conclusion
Large cervical teratomas pose significant and profound management challenges in resource constrained settings. In order to avoid delay in treatment or inadequate treatment, concerted efforts must be made to confirm the diagnosis of cervical neck swellings and early complete surgical excision offered. Thorough periodic physical examinations and ultrasound scan of the neck is recommended for mature cervical teratoma patients in resource constrained environments.
REFERENCES
1.
Paradies G, Zullino F, Orofino A, Leggio S. Mediastinal teratomas in children. Case reports and review of the literature. Ann Ital Chir 2013;84(4):395–403.
[Pubmed]

2.
Ali IM, Yaşar M, Abdi AA, Dirken ES. Successful surgical management of a giant neck teratoma in a newborn baby: A case report. Ann Med Surg (Lond) 2022;82:104694. [CrossRef]
[Pubmed]
3.
Mukhopadhyay M, Mandal KC, Das C, Mukhopadhyay B, Mukhopadhyay B, Halder P. Extra-gonadal teratomas in atypical sites in neonates and children – Our experience and review of the literature. Clin Oncol Res 2021;4(2):2613–4942. [CrossRef]
4.
Paradies G, Zullino F, Orofino A, Leggio S. Rare extragonadal teratomas in children: Complete tumor excision as a reliable and essential procedure for significant survival. Clinical experience and review of the literature. Ann Ital Chir 2014;85(1):56–68.
[Pubmed]
5.
Milsten J, Weitkamp SA, Aghte AG, Weitkamp JH. Giant congenital cervical teratoma: A case report. J Pediatr Surg Case Reports 2025;112:102938.
6.
Patel S, Kunnath AJ, Gallant JN, Belcher RH. Surgical management and outcomes of pediatric congenital head and neck teratomas: A scoping review. OTO Open 2023;7(3):e66. [CrossRef]
[Pubmed]
7.
Hochwald O, Gil Z, Gordin A, Winer Z, Avrahami R, Abargel E, et al. Three-step management of a newborn with a giant, highly vascularized, cervical teratoma: A case report. J Med Case Rep 2019;13(1):73. [CrossRef]
[Pubmed]
8.
Wolter NE, Siegele B, Cunningham MJ. Cystic cervical teratoma: A diagnostic and management challenge. Int J Pediatr Otorhinolaryngol 2017;95:97–100. [CrossRef]
[Pubmed]
9.
Abdur-Rahman LO, Baba S, Bamigbola KT, Olaoye I, Oyinloye AO, Nasir AA, et al. Outcome of management of complicated extragonadal teratoma in a resource poor setting. Afr J Paediatr Surg 2013;10(4):323–6. [CrossRef]
[Pubmed]
10.
Gezer HÖ, Oğuzkurt P, Temiz A, Bolat FA, Hiçsönmez A. Huge neck masses causing respiratory distress in neonates: Two cases of congenital cervical teratoma. Pediatr Neonatol 2016;57(6):526–30. [CrossRef]
[Pubmed]
11.
Malhotra S, Negi P, Sagar P. A case of cervical teratoma in an infant. Indian J Otolaryngol Head Neck Surg 2022;74(Suppl 3):6519–23. [CrossRef]
[Pubmed]
12.
Olivares E, Castellow J, Khan J, Grasso S, Fong V. Massive fetal cervical teratoma managed with the ex utero intrapartum treatment (EXIT) procedure. Radiol Case Rep 2018;13(2):389–91.
[Pubmed]
13.
Neff L. Cervical teratomas. Oper Tech Otolaryngol Head Neck Surg 2017;28:190–5.
14.
Głowska-Ciemny J, Szymanski M, Kuszerska A, Rzepka R, von Kaisenberg CS, Kocyłowski R. Role of alpha-fetoprotein (AFP) in diagnosing childhood cancers and genetic-related chronic diseases. Cancers (Basel) 2023;15(17):4302. [CrossRef]
[Pubmed]
15.
Paradis J, Koltai PJ. Pediatric teratoma and dermoid cysts. Otolaryngol Clin North Am 2015;48(1):121–36. [CrossRef]
[Pubmed]
16.
Hadley LGP, Rouma BS, Saad-Eldin Y. Challenge of pediatric oncology in Africa. Semin Pediatr Surg 2012;21(2):136–41. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Akputa Aja Obasi - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Wilson Egwu Sunday Omebe - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Iniofon Clement Akpaette - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Akputa Aja Obasi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}